A study to explore the need for and feasibility of implementing supervised consumption services in the City of Greater Sudbury
“We respectfully acknowledge the traditional territory of Atikameksheng Anishnawbek and Wahnapitae First Nation, as well as the Robinson- Huron Treaty on which this study was conducted. These lands encompass strong and vibrant communities of the Anishinabek and the many other Indigenous Peoples who reside in these communities. Their enduring presence and resilience is felt throughout our shared history and in present day. We strive for respectful relationships with all Indigenous Peoples. We are committed to honour our shared history and ensure healthier communities for all.”
Executive summary
The Community Drug Strategy for the City of Greater Sudbury undertook a study to determine the need for and the feasibility of implementing supervised consumption services (SCS), in Greater Sudbury. Supervised consumption services are monitored spaces where people can consume drugs under supervision with sterile supplies. The study was completed between April 2019 and June 2020. The study consisted of a survey with people who inject drugs (PWID), a survey of Greater Sudbury community members, focus groups with community partners and stakeholders, and secondary data analysis.
The City of Greater Sudbury would benefit from supervised consumption services.
Although there are existing harm reduction services in Greater Sudbury, the health harms associated with injection drug use are significant and rising. Sudbury and districts i (2018) ranked twelfth in the province for opioid-related emergency department visits, seventh in the province for confirmed opioid-related deaths, and tenth for hospitalizations, based on rates per 1000 population. The frequency of emergency medical service (EMS) calls for suspected opioid overdose have more than double in 2019 compared with 2018. Three-quarters (75.0%) of respondents from the survey of people who inject drugs (PWID) said they had injected drugs in public. More than half had overdosed in their lifetime.
From the perspectives of law enforcement and health care providers, drug and substance use creates pressures on social services, police, paramedic, and hospitals. The need for EMS workers and police officers at overdose sites means that they are pulled away from other community needs.
Supervised consumption services may be a feasible strategy for the City of Greater Sudbury, but there are some concerns that need to be addressed.
Potential clients (89.0%) say they would use SCS if available and among community survey respondents, 59.8% believed that these services would be helpful in Greater Sudbury. All three groups of study respondents identified that the greatest benefits of SCS would be the prevention and treatment of accidental overdoses and the ability to access sterile injection equipment.
Additional benefits identified by all three groups of study respondents include less public drug use on streets or in parks, fewer used needles on the streets or in parks, and less risk of injury and death from drug overdose. Concerns expressed in the community survey were related to neighbourhood safety, an increase in crime and drug use, and more drug dealers targeting the area. Although some respondents did not support the idea of SCS and did not respond to the question about mitigation strategies, others felt that some concerns could be addressed through strategies such as evaluating the services, sharing results with the community, and then taking action (58.2%), providing information about the goals and benefits of SCS (48.7%), and having a community group to work on issues about SCS (33.9%).
If SCS are considered in Greater Sudbury, all those consulted suggested that a location should be carefully chosen. The most common suggestion was a centralized location in the downtown core, in proximity to, and integrated with, existing harm reduction services and the majority of health care and social services. A mobile service was also proposed by some respondents.
i When Greater Sudbury data are not available, data from Sudbury and districts are used.
Highlights
Supervised consumption services (SCS) are monitored spaces where people can consume drugs under supervision in an environment with sterile supplies.
The Community Drug Strategy for the City of Greater Sudbury undertook a study to determine the need for and the feasibility of implementing SCS. The study consisted of a peer-led survey with 190 people who inject drugs (PWID), an online survey responded to by 2251 Greater Sudbury community members, and focus groups with 52 community partners and stakeholders. In addition to these primary sources of information, the researchers also consulted secondary data on population health information, drug use, opioid harms, prescription patterns, opioid toxicity, and opioid overdoses.
The City of Greater Sudbury would benefit from supervised consumption services.
- For 2018, per 1000 population, Sudbury and districts ranked twelfth in the province for opioid-related emergency department visits, seventh in the province for confirmed opioid-related deaths, and tenth for hospitalizations. Within Sudbury and districts, there were 199 opioid-related deaths between 2010 and 2018.
- The negative health outcomes are increasing: The frequency of emergency medical service (EMS) calls for suspected opioid overdose was higher in 2019 (468 calls) compared to 2018 (200 calls). Deaths due to opioid-related overdoses in Sudbury and districts increased in 2019, with approximately the same number of deaths in the first half of 2019 (28 deaths) as were experienced in all of 2017 (34 deaths) or 2018 (32 deaths).
- People who inject drugs do so frequently; 43.0% of PWID survey respondents inject several times per day.
- Drugs mixed with other substances can pose a risk because the user may experience an unexpected or adverse reaction. The majority of PWID surveyed, 85.2%, indicated that they have taken a drug they believed was mixed with another substance.
- Accidental overdose is a common experience among PWID in Greater Sudbury. Among the PWID surveyed, more than half had accidentally overdosed in their lifetime. Injecting drugs alone poses increased risk of adverse consequences. The large majority of PWID surveyed (83.2%) said that they have injected alone.
- Injecting in public may demonstrate that there is a need for designated supervised space for injecting. Three-quarters (75.0%) of respondents said they had injected drugs in public.
- One-third of respondents (32.6%) indicated they have used a needle previously used by someone else, placing them at greater risk of contracting blood borne infections such as HIV and Hepatitis C.
From the perspectives of law enforcement and health care providers, drug use creates pressures on social services, police, paramedic, hospitals. The need for EMS workers and police officers at overdose sites means that they are pulled away from other community needs.
Supervised consumption services may be a feasible strategy for the City of Greater Sudbury, but there are some concerns that would need to be addressed.
The majority of PWID (89.0%), indicated that they would be willing to use SCS. Among those PWID who would use SCS, their single most important benefit was access to sterile injection equipment (27.5%), or that overdoses can be prevented (20.9%) or treated (20.3%).
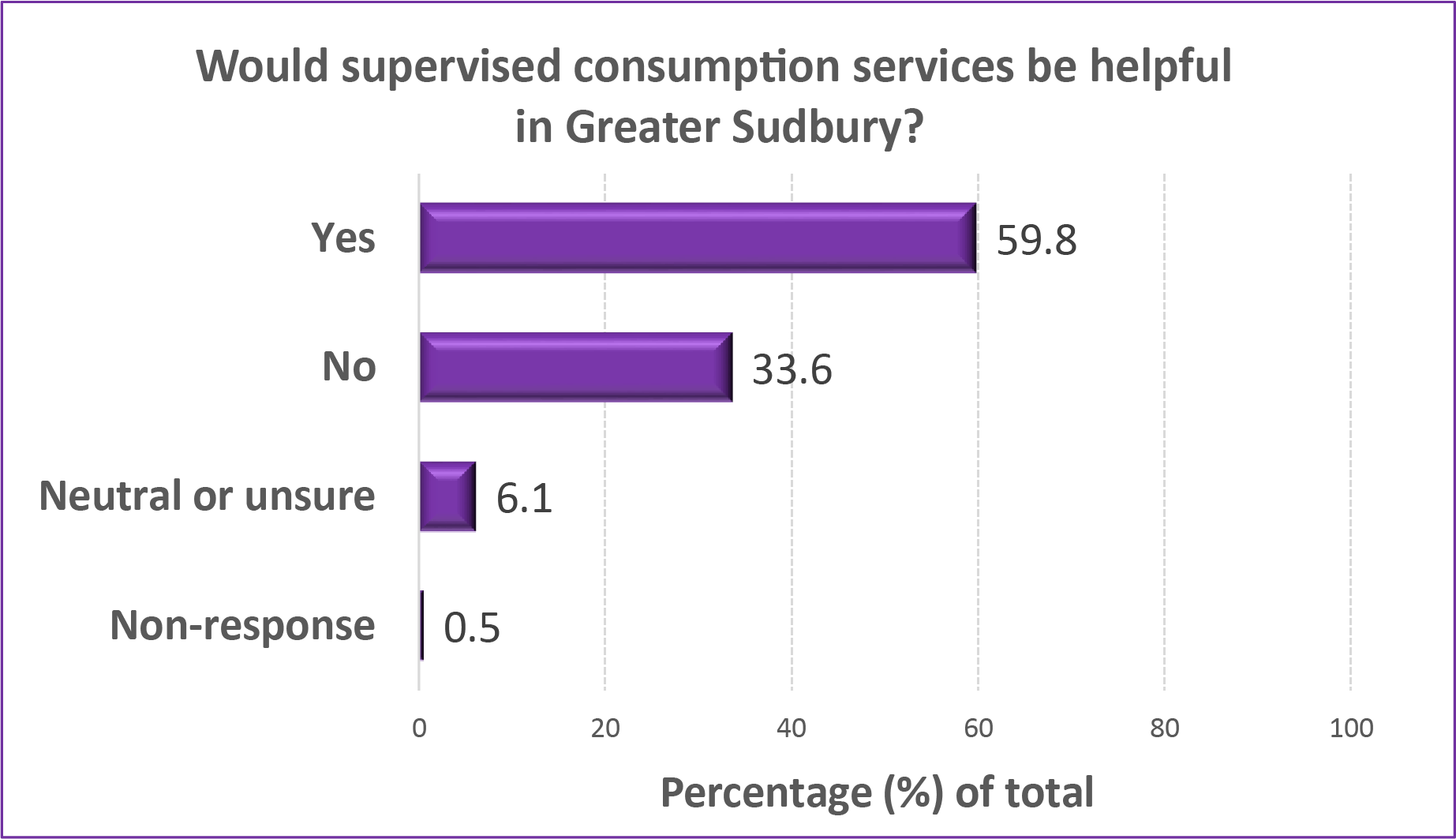
Among community survey respondents, 59.8% believed that these services would be helpful in Greater Sudbury, while 33.6% of respondents did not believe these types of services would be helpful, and 6.1% were neutral or unsure.
Stakeholders identified benefits for people who inject drugs, the community and services.
“The benefits of having a SCS is that it’s located in one area, access to other services, so whether it’s drug information or access to other social workers or nurses, or people, I guess ultimately the idea is that if you got a user in front of you, you can try and help them.”
The following potential benefits were identified by community respondents:
- less public drug use on streets or in parks (62.3%)
- fewer used needles on the streets or in parks (62.3%)
- less risk of injury and death from drug overdose (60.1%)
There are concerns and challenges associated with supervised consumption services
Although 89.0% of PWID indicated that they would make use of SCS, those who responded that they would not use these services, or may not use them frequently, expressed concerns about anonymity and fear of police, or noted that they were self-sufficient and not in need of these services.
Business owners and community members expressed concerns about negative impacts around the area of SCS, with effects on perceived neighbourhood safety and desirability, a potential increase in crime and drug use, and more drug dealers targeting the area. Approximately one-third of survey respondents had concerns that SCS could lead to more drug use, more drug selling or trafficking in the area, and more people who use drugs in the area.
There are possible mitigation strategies to address the concerns
It was felt by some focus group participants that many concerns are due to lack of knowledge about the benefits and effectiveness of SCS and lack of understanding about mental health/illness and the link to addiction, and that increased awareness could mitigate some of the concern. Community residents felt that some common mitigation strategies could be helpful:
- Provide information about the goals of SCS and how they can help the community.
- Have a community group to work on issues about SCS.
- Evaluate the services, share results with the community, and take action.
Supervised consumption services should be integrated with existing services
Focus group participants said it was important to build on existing harm reduction programs in Greater Sudbury. Organizations that offer these programs were identified as having the appropriate approach/model to support the needs of those who would use SCS and the needs of the larger community.
If supervised consumption services are considered, the most appropriate location(s) should be carefully chosen
Community survey respondents had concerns about locating SCS in close proximity to schools or other community locations occupied by children. If SCS are considered, PWID were most likely to suggest the downtown core of Sudbury (65.8%) among possible locations. In general, among those who would consider SCS as an option, focus group participants and community survey respondents suggested one SCS site, located in a centralized location in the downtown core, although a mobile site was also suggested to provide services closer to wherever users live. The majority of health care and social services are located in the downtown core, and a downtown location would be in close proximity these supports.
Foreword
Substance use impacts everyone. The rates of illicit drug use continue to be higher in Greater Sudbury than those for Ontario overall, and impact the health and safety of our communities. Based on rates per 1000 population for 2018, Sudbury & districts ranked twelfth in the province for opioid-related emergency department visits, seventh in the province for confirmed opioid-related deaths, and tenth for hospitalizations. Addressing the individual and societal issues associated with drug use requires the cooperation and collaboration of many community partners and private citizens. It is a multifaceted approach that requires diverse voices to help inform decisions.
The people impacted by substance use deserve a comprehensive approach to service delivery that is grounded in compassion and evidence. Public Health Sudbury & Districts and the Greater Sudbury Police Service, on behalf of the Community Drug Strategy for the City of Greater Sudbury, are pleased to share the final report of the Supervised Consumption Services Needs Assessment and Feasibility Study. The findings of the study inform local direction about supervised consumption services. These services are one component of our comprehensive strategy to protect the health of our community and reduce harms associated with drug use.
The study itself provided the community with opportunities to become meaningfully engaged and involved in the development, delivery, and evaluation of programs that are intended to serve them. We would like to acknowledge and thank the many people that took part in the community survey; those with lived experience who shared their important perspectives; and the health and social services agencies, friends and family of people who inject drugs, the business community, and local community organizations who all engaged in targeted focus groups. This report is a culmination of the voices of our community—working together to improve the health, safety, and wellbeing of all individuals, families, neighbourhoods, and communities in Greater Sudbury.
We would also like to take this opportunity to thank the many researchers, policy experts, service providers, and community partners who have given so generously of their time and expertise to support the development of this report. And to all the members of the Community Drug Strategy for the City of Greater Sudbury— thank you for your ongoing support in this important work. We look forward to our continued efforts to provide access to appropriate, effective and acceptable services, and resources in our community. Together we will continue to build a healthier and safer community by lessening the harms associated with substance use.
| Dr. Penny Sutcliffe, MD, MHSc, FRCPC Medical Officer of Health/CEO Public Health Sudbury & Districts | Paul Pedersen, M.P.A., Dip.ED, C.M.M. III, C.M.I. VII Chief of Police Greater Sudbury Police Service |
Introduction
Supervised consumption services (SCS) are controlled spaces where people can consume drugs under supervision with sterile supplies. Spaces are supervised by trained staff, including health care professionals. People who use the service can also receive basic medical care and referrals to other health and social services1. SCS do not provide drugs to people. These services are legal in Canada with federal and provincial government approval2. SCS have been shown to reduce the mortality and morbidity associated with injection drug use, including infection and death3.
In the City of Greater Sudbury, the first comprehensive report “Community Drug Strategy for the City of Greater Sudbury: A Call to Action4 was released in 2015, focusing on health promotion and prevention, treatment, harm reduction, and enforcement and safety. Since that time, the Community Drug Strategy for the City of Greater Sudbury, representing more than 25 community partners from community agencies including health, social services, education, police, justice and emergency services, have been actively working to improve community health and address drug-related issues by increasing public awareness of drug use as a health issue5. In 2018, the need to understand potential strategies to reduce drug-related harms, without requiring the cessation of drug use, was identified.
As noted in an evidence review by the British Columbia Centre on Substance Use6, evaluation research on SCS consistently demonstrates the following outcomes: reducing morbidity and mortality associated with overdose7,8,9,10; reducing risk for infectious disease transmission and increase harm reduction practice such as reduction in syringe reuse11,12,13,14,15,16,17,18; “improving contact between a highly marginalized ‘at-risk’ population and the health care system”19; enhancing recruitment into medical care and addiction treatment and withdrawal management20,21,22,23,24,25,26,27 and methadone therapy28,29,30,31,32; reducing pressures on emergency services33; reducing public drug use34,35, syringes discarded in public, and other injection-related litter36,37,38.
While there have been concerns that SCS encourage and foster drug use, there has been no increase in the number of people using drugs intravenously in localities where such facilities operate39. Further, evaluation work undertaken in Vancouver revealed that the opening of Insite was not associated with increased crime or rates of initiation into injection drug use40,41. These facilities have also been found to be highly cost-effective42,43.
Research purpose and objectives
The overall purpose of this study was to determine the need for and the feasibility of implementing SCS in the City of Greater Sudbury, from the perspective of all community stakeholders (including people who inject drugs, Greater Sudbury residents, community partners, and other key stakeholders).
Specifically, the study addressed the following objectives:
- Determine the need for SCS in the City of Greater Sudbury;
- Determine the conditions under which SCS would be used and judged as suitable or attractive by program deliverers and potential clients;
- Determine the extent to which SCS are seen as helpful by community stakeholders and the community;
- Identify concerns/challenges/barriers that might be associated with SCS in Greater Sudbury and discuss potential mitigation strategies to address them;
- Determine how SCS could be integrated with existing harm reduction services in Greater Sudbury; and
- Determine potential locations for SCS.
This report summarizes the findings related to each objective.
Data collection methods
Needs and feasibility studies of SCS from similar-sized communities in Ontario, such as Thunder Bay44, London45, and Waterloo46, were reviewed in the development of surveys and focus group questions for this study. Ethics approval for all parts of this research was received from the Public Health Sudbury & Districts Research Ethics Review Committee and the Health Sciences North Research Ethics
Board.
Public Health Sudbury & Districts led the study on behalf of the Community Drug Strategy for the City of Greater Sudbury. The study was supported by the City of Greater Sudbury, the North East Local Health Integration Network, the Canadian Mental Health Association, and Public Health Sudbury & Districts. A Community Advisory Committee and a Research and Technical Working Group provided guidance on the study. A Northern Ontario School of Medicine (NOSM) research team collected the data, and analyses were completed by NOSM and Public Health Sudbury & Districts.
The following primary data collection methods were used to address the research objectives:
- a peer-led survey with people who injected drugs within the last six months
- a community online survey
- focus groups with community partners, including those working in harm reduction, health promotion, treatment, enforcement and justice, local businesses, non-profit and other community organizations, and family and friends of people who inject drugs
In addition to these primary sources of information, the researchers also consulted secondary data on population health information, drug use, opioid harms, prescription patterns, opioid toxicity, and opioid overdoses.
Respondents
People who inject drugs (PWID) survey participants
This peer-led survey with people who inject drugs was conducted throughout the month of July 2019. A total of 190 participants completed all or a portion of the survey; all participants had injected drugs within the previous 6 months prior to the survey, were at least 16 years of age, and were able to give free and willing consent to participate.
Approximately 60% were male, and the mean age of respondents was 40 years (with a range from 17 to 66 years); 88.4% spoke English as a first language; 86.3% reported being heterosexual; and 25.8% reported having any university/college as highest level of education. The majority of PWID in this study either identified as Indigenousii (55.8%) or as Caucasian (42.1%). Although participation in the survey required all participants to have injected drugs within 6 months prior to the study, 86.8% reported using injection drugs in the previous 30 days.
Focus group participants
Focus group participants were largely identified through membership in the Community Drug Strategy for the City of Greater Sudbury. A total of 52 community stakeholders participated in 13 focus groups held between September to November 2019, representing the following sectors and perspectives: addiction treatment (n=11); enforcement and justice (n=4); health promotion and prevention (n=11); harm reduction (n=7); business sector and other community organizations (n=10); and friends and family of people who inject drugs (n=9).
Community survey participants
The community survey was available online through the Community Drug Strategy for the City of Greater Sudbury website from June through September 2019; paper copies were also available at community partner locations until the survey closed online. A total of 2251 respondents completed all or a portion of the survey; all respondents indicated they were at least 16 years of age, and were able to give free and willing consent to participate.
Among the 2251 respondents, 62.5% identified as female, and 55.0% of respondents were between 25 to 44 years of age. Of the respondents, 19.8% reported working in health care or being a first responder, 12.7% worked in the harm reduction field, and 6.3% reported being a business owner.
ii We recognize First Nations, Métis and Inuit as three distinct cultural identity groups, each of which has a unique history, set of traditions and cultural practices, and governance structures. For the purpose of this document the term Indigenous will be used to encompass these populations. However, the term First Nations community will be used when referring to communities located on reserve.
Findings
Context
The City of Greater Sudbury
The City of Greater Sudbury is located in Northeastern Ontario on the Canadian Shield about 400 kilometres north of Toronto47. With a population of approximately 162 000 living in a mix of urban, rural, and wilderness environments, it is the largest and most populated centre north of the Greater Toronto Area48. Greater Sudbury is geographically the largest municipality in Ontario, encompassing 3228 square kilometres49. It is a multicultural community, with 27.0% of the population reporting French as their mother tongue50. As per the Greater Sudbury census metropolitan area, Greater Sudbury is located on the territories of two First Nation communities, Wahnapitae First Nation and Atikameksheng Anishnawbek and is home of approximately 9.0% of people who identify as Indigenous, some of which are First Nation members of other First Nation communities51.
In 2016, 13.0% of the population of Greater Sudbury were living in povertyiii,52. A 2018 point-in-time count reported 1954 individuals who identified as either absolutely homeless, hidden homeless or at-risk of homelessness; an additional 224 were dependent children under the age of 18, of whom participants had custody53. One of the top reasons reported for homelessness was addictions54. Compounding homelessness, Greater Sudbury has a 5-year wait time for a one-bedroom subsidized unit, and a wait list of over 1000 residents for geared-to-income housing55.
Current local harm reduction responses and usage
In the City of Greater Sudbury, several harm reduction strategies have been implemented to increase the safety and health of the community related to substance use.
- The Needle Exchange Program (NEP, also known as The Point) is a free and confidential program that provides harm reduction supplies and services to people who use drugs, including provision of new needles, needle pick-up and disposal bins56. It aims to reduce the risks of getting or passing on infectious diseases, such as HIV and hepatitis C, and reduce risks associated with using drugs. In 2019, 1 495 919 needles were distributed through the NEP, including the fixed site at the Rainbow Mall and through outreach services across Sudbury and districts57. There were 900 visits to the Needle Exchange Program in 201958.
- Pre-assembled naloxoneiv spray kits are distributed to NEP clients who are at risk of opioid overdose and to friends and family members of those at-risk59. Naloxone is also distributed to eligible agencies and pharmacies to distribute to clients as part of the Ontario Naloxone Program. In Greater Sudbury, Public Health Sudbury & Districts, Réseau ACCESS Network, and pharmacies receive naloxone through this program. Training related to naloxone storage, administration and distribution is provided through the Naloxone Distribution Program by Public Health Sudbury & Districts to eligible agencies and is ongoing in the community. In addition, Réseau ACCESS Network provides training on naloxone storage and administration and distributes kits to those most at risk for overdose.
- Since May, 2019, the Sudbury Temporary Overdose Prevention Society (STOP Society) has offered periodic unsanctioned SCS at five pop-up sites in Greater Sudbury’s downtown core60. They do not have a federal exemption to operate. STOP offers clients and the community the following services: community clean-up; harm reduction teaching; brief counselling; Indigenous traditional services; practical support; grief counselling; and medical care. Additionally STOP has provided referrals to the following: addiction services; harm reduction services; clinical service providers; mental health service providers; and other community-based service providers61. Over a seven month period, from May to November, 2019, STOP provided a total of 14 operational days and assisted a total of 140 clients62.
- The Sudbury Action Centre for Youth (SACY), in partnership with Laurentian University, offers a drug testing program63. A spectrometer is used to assist in drug identification. As of March 2019, there were 10 samples being tested per month. SACY also provides harm reduction services in the form of outreach and the provision of supplies and services to promote clean and safe use of drugs64.
- As part of the Community Drug Strategy, Public Health Sudbury & Districts has been issuing drug alerts and warnings since 201765. The alerts and warnings are issued to notify the community of increased opioid-related incidents or of new toxic drug trends in Greater Sudbury. The alerts are released as a result of ongoing data surveillance, ministry notices, and information from community partners. Since its inception to May 2020, 12 drug alerts have been issued in the City of Greater Sudbury66.
- Police Services: the Greater Sudbury Police Service (GSPS) has implemented visibility strategies to address issues in the downtown core. In 2018 to 2019 there has been a 14.0% increase in downtown bike patrols67. GSPS continues to target enforcement towards drug suppliers, employs drug recognition experts, provides education and issuance of naloxone and supports advocacy efforts for appropriate sentencing as it relates to illicit drug suppliers and users.
- Mobile Crisis Response Program: the Program is in association with the Crisis Intervention Program, Greater Sudbury Police Service, Greater Sudbury Paramedic Services, and Health Sciences North’s Emergency Department68. Various health services such as health checks and mental health and addiction supports are provided in social settings (e.g. housing buildings, and shelters) to best meet the needs of individuals.
- Rapid Mobilization Table (RMT): Community Mobilization Sudbury (CMS) comprises 25 partner organizations from diverse sectors such as health, children’s services, policing, education, mental health and addictions, housing, and municipal services that coordinate to utilize existing systems and resources69. Representatives from CMS partners meet twice each week at the RMT. Participants collaboratively identify situations involving those who are at high risk of harm. All necessary agency partners participate in a coordinated, joint response – ensuring that those at risk are connected to appropriate, timely, effective, and caring supports.
- Canadian Mental Health Association’s Harm Reduction Home Residential Program works to support individuals who are homeless or at risk of homelessness and who are also impacted by alcohol dependence70. The program provides access to a managed alcohol program where individuals are supported with housing and addressing primary care and mental health needs.
- Ontario Aboriginal HIV/AIDS Strategy provides outreach and support to Indigenous people who use drugs71. They provide free access to sterile drug use supplies, while supplying traditional medicines and resources to access traditional supports through community networks.
- Réseau ACCESS Network provides harm reduction services through The Street Outreach Program, which operates seven days a week72. Outreach workers provide safe injection/inhalation supplies, referrals to addiction treatment centres, testing services, HCV treatment, referrals for HIV treatment, support and counselling and advocacy and accompaniment. Their outreach includes education to prevent harms of drug use, naloxone training and distribution, and distribution of safe supplies.
- Shkagamik-Kwe Health Centre is an Aboriginal Health Access Centre, which provides community-based programs that are delivered in a culturally safe environment free of judgment73.
From the people who inject drugs (PWID) survey, it is evident that many of the existing harm reduction services in Greater Sudbury are accepted and well-used. In addition, there continue to be gaps and resource limitations.
- 76.8% of PWID indicated that they have exchanged or obtained needles through existing services in Greater Sudbury in the last 6 months.
- 93.2% of PWID were aware of take-home naloxone kits, and of those, 78.8% had their own kits. PWID indicated they had obtained naloxone kits through a methadone clinic (39.1%), the needle distribution program (38.3%), from outreach workers (36.2%), or a pharmacy (18.5%).
- Knowledge of naloxone was also demonstrated to come from existing services, with PWID indicating they had learned about naloxone from outreach workers and street nurses (45.8%), the needle distribution program (19.2%), or through a methadone clinic (18.1%).
- 55.5% of PWID accessed blood testing services for HIV, and 54.7% for hepatitis C (Hep C), from a wide range of local service providers including Public Health Sudbury & Districts, Health Sciences North, Réseau ACCESS Network, jail, pharmacies, and Indigenous programs.
- 74.7% of PWID indicated that they had been in a drug treatment program during their lifetime, and 60.0% indicated that they had been in a detox program.
- 29.5% of PWID had tried to access treatment programs but were unable.
iii The Low-income measure after tax (LIM-AT) is a fixed percentage (50%) of median adjusted after-tax income of households observed at the person level, where ‘adjusted’ indicates that a household’s needs are taken into account.
iv Naloxone can temporarily reverse the effects of an opioid overdose that may cause a person to stop breathing.
Need for supervised consumption services
Determining the need for SCS in Greater Sudbury was the primary objective of this research study. The following results describe aspects of the need for supervised consumption services in Greater Sudbury from the perspectives of people who inject drugs, key stakeholders, and Greater Sudbury community members. Indicators of need for SCS may include a sizable population that injects drugs; unsafe injection practices; significant negative outcomes such as overdoses, ER visits and hospitalizations; impact on emergency services and law enforcement; existing harm reduction supports, such as needle exchange programs that can complement SCS; gaps in support and referral options; and social and family
impacts of injection drug use74,75,76,77.
Drug use in the City of Greater Sudbury
Harm reduction services, including needle and naloxone distribution, are already implemented in the City of Greater Sudbury. Distribution of needles remained constant between 2013 and 2016 at approximately 500 000 distributed needles annually. However, in 2018 the number of distributed needles increased dramatically to 1.5 million78. Since July 2018, Public Health Sudbury & Districts staff have trained 413 individuals from 63 community organizations to administer naloxone79. In 2019, Public Health Sudbury & Districts distributed a total of 6958 naloxone kits and refills to community agencies, while Réseau ACCESS Network and pharmacies distributed a further 3052 and 6438 kits and refills, respectively80.
1.5 million
needles distributed in the City of Greater Sudbury in 2018.
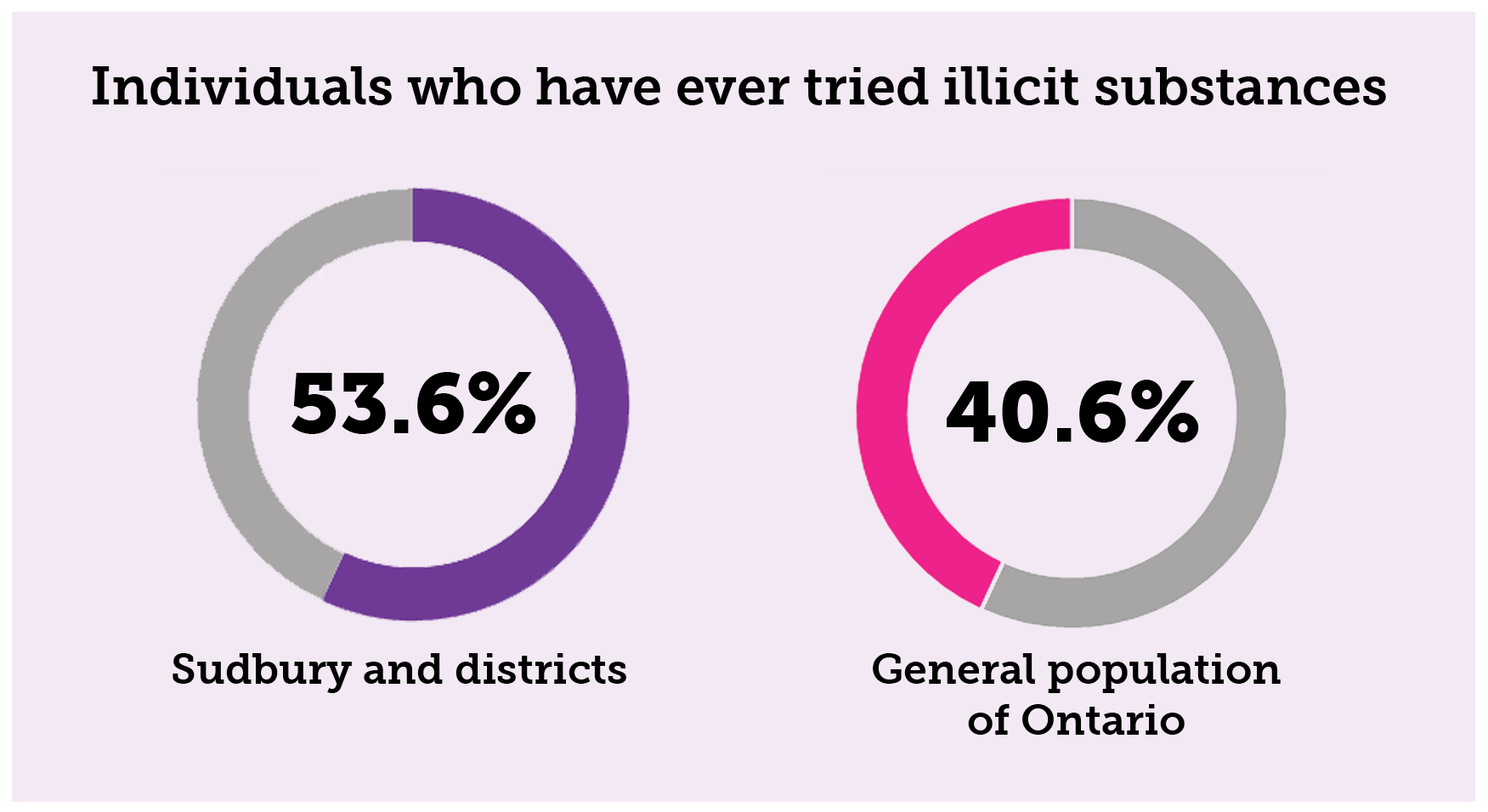
Although there are existing harm reduction services in Greater Sudbury, the health harms associated with drug and substance use are significant and rising81. There is a significantly higher proportion of individuals who have ever tried illicit substances in Sudbury and districts compared to the general population of Ontario; 53.6% compared to 40.6% respectively82. Based on Canadian Community Health Survey data from 2015 to 2017, it is estimated that in 2019 there were 1817 (95% CI 840–2795) adults in Greater Sudbury who have used illicit drugs (such as cocaine, amphetamines, opioids or hallucinogens), excluding adults using cannabis83.
Figure 1: Individuals who have tried illicit substances in Sudbury and districts and in Ontario (%)
In 2018, per 1000 population, Sudbury & districts ranked twelfth in the province for opioid-related emergency department visits, seventh in the province for confirmed opioid-related deaths, and tenth for hospitalizations84. In 2018, Public Health Sudbury & Districts area was the eleventh highest Public Health region for opioid prescribing for overall and new individuals, with a rate of 140.6 per 1000 population85. Within Sudbury and districts, there were 199 opioid-related deaths between 2010 and 201886.
199
opioid-related deaths between 2010 and 2018 within Sudbury and districts.
The frequency of emergency medical service (EMS) calls for suspected opioid overdose was higher in 2019 (n=468) compared to 2018 (n=200), and was higher in every month87.
Deaths due to opioid-related overdoses in the Sudbury and districts increased in 2019, with approximately the same number of deaths in the first half of 2019 (28 deaths) as were experienced in all of 2017 (34 deaths) or 2018 (32 deaths)88.
Opioid-related toxicity and opioid-related deaths disproportionately affect Ontario’s Indigenous populations and more greatly impact Indigenous people living off a First Nations community89. Recent data demonstrate that the rate of opioid related toxicity (both emergency department visits and hospitalizations) is almost 4.5 times higher for Indigenous people living off a First Nations community and almost 2.5 times higher for Indigenous people living on a First Nations community compared to the general population90. Moreover, the rate of opioid-related mortality is 4.25 times higher for Indigenous people living off a First Nations community and 2.25 times higher for Indigenous people living on a First Nations community compared to the general population91. The greater inequities observed by these data exist in a context of colonization, historical and current trauma, and systemic racism. First Nations communities are at a higher risk of experiencing opioid-related morbidity and mortality due to the intergenerational impacts of colonialism, including residential schooling and the historical erosion of First Nations culture92.
From the perspective of people who inject drugs
Living situation
The large majority of people who inject drugs (PWID) survey respondents (91.6%)
lived in Greater Sudbury. In terms of housing, 43.4% reported that during the last 6 months, the place they lived most of the time was in their or their partner’s house or apartment; 12.7% indicated that they lived where people gather to use drugs (e.g., a crack house), 38.0% of PWID respondents reported being homeless in the past 6 months.
Two-thirds of respondents (67.4%) lived below the poverty line/low income threshold (broken down, 38.4% earned less than $10,000 in the previous year and 29.0% earned between $10,000 to $19,999), while 11.6% earned between $20,000 to $29,999; only 9.0% earned $30,000 or more. Additionally, 8.9% reported having a regular job, 11.0% reported being temporarily employed, and 11.0% being self-employed. The most common source of income was Ontario Works (OW) (42.6%), followed by Ontario Disability Support Program (ODSP) (38.9%), and GST rebates (14.7%). Some respondents reported criminal activity as sources of income: 21.6% reported selling drugs, 16.3% reported theft/robbery/stealing, while 9.5% reported each of the following activities: selling sex, cigarettes/tobacco, and other criminal activities.
Drug use
The average age when survey respondents began using drugs was 22 years (with a range between 9 to 40 years) (among those 93 respondents who answered this question).
Survey respondents who inject drugs do so frequently, with almost two-thirds (66.8%) reporting that they used injection drugs on a daily (43.2%) or weekly (23.7%) basis, while the remainder of respondents indicated that they used injection drugs on a monthly or less frequent basis (24.2%). On average, for those who responded on frequency of injecting during a day (n=105), 94.3% inject drugs multiple times a day; only 5.7% of users reported injecting once during the day. Others indicated that they injected on average 3 times a day (10.5%), 4 times (9.5%), 5 times (11.4%) or more than 10 times per day (22.0%).
Types of drugs used
A variety of drugs are consumed by people who use drugs in Greater Sudbury. Cocaine is the most common drug of choice, with ‘hydros’ (e.g., HydroMorphone, Contin, Dilaudid), crack, heroin, fentanyl, morphine, amphetamines, crystal meth, and speedballs as other drugs of choice. Overall, opioids are slightly more consumed than stimulants.
Table 1: Drugs most often injected during the last six months (more than one response permitted)
| Drug Classification | Drug | Frequency | Percent |
|---|---|---|---|
| Opioids | Hydros | 62 | 32.6% |
| Heroin | 44 | 23.2% | |
| Fentanyl | 38 | 20.0% | |
| Morphine | 26 | 13.7% | |
| Methadone (prescribed) | 9 | 4.7% | |
| Percocet | 6 | 3.2% | |
| Oxy Neo | 5 | 2.6% | |
| Oxycodone | 4 | 2.1% | |
| Methadone (not prescribed) | 3 | 1.6% | |
| Total | 197 | ||
| Stimulants | Cocaine | 90 | 47.4% |
| Crack/rock cocaine | 30 | 15.8% | |
| Crystal meth | 20 | 10.5% | |
| Amphetamines (speed) | 20 | 10.5% | |
| Speedball | 13 | 6.8% | |
| Ritalin or Biphentin | 6 | 3.2% | |
| Total | 179 | ||
| Tranquilizers or Benzos | Total | 5 | 2.6% |
| Anti-depressants | 0.0% | ||
| Wellbutrin - Total | 5 | 2.6% | |
| Gabapentin | Total | 1 | .05% |
Drugs mixed with other substances
Drugs mixed or ‘cut’ with other substances can pose a risk because the person who is using the substance may experience an unexpected or adverse reaction. The majority of PWID surveyed, 85.2%, indicated that they have taken a drug they believed was cut with another substance; of these, 88.1% believe they have done so in the last 6 months.
Experiences of overdose
Accidental overdose is a common experience among PWID in Greater Sudbury. Among the PWID surveyed, more than half (53.7%) said they had overdosed in their lifetime, and of these, 58.8% had experienced 1 or more overdoses in the last 6 months. The majority (84.3%) of the PWID who had experienced an overdose were with other people at the time: an intimate partner (36.3%), a close friend (29.4%), a casual acquaintance (19.6%), or a stranger (17.6%). In terms of location, 41.2% of overdoses occurred in their own home, 19.6% occurred at a friend’s place, while 11.8% reported an overdose in the street (alley, doorway, etc.).
Of the respondents who had experienced an overdose during their lifetime, 84.3% reported receiving help during an overdose, while 15.7% did not. More than half (54.9%) reported that an ambulance was called and of these, 76.8% were taken to the hospital.
Almost two-thirds of PWID (61.2%) have administered naloxone to someone who was experiencing an overdose, most doing so more than once.
Injection practices
Access to sterile needles and equipment
Reusing and sharing needles increases the risk of acquiring blood-borne infections through injection drug use93. Reported reuse or sharing of equipment may indicate a need for access to a reliable source for sterile equipment, such as could be provided at a SCS. Approximately three-quarters of PWID in the survey (71.1%) said that they have reused a needle (see Figure 2 for frequency of reusing).
Figure 2: Frequency of reusing needles (among those who ever reuse) (%)
In addition, one-third of respondents (32.6%) indicated they have used a needle previously used by someone else. More than one-third of respondents (38.4%) indicated they have used other previously-used injecting equipment (cotton, filter, spoon, cooker), and 36.3% said that they have used puddle water or other nonsterile water source.
More than three-quarters (80.5%) of PWID survey respondents have obtained sterile needles from a friend, 76.4% have used a local needle distribution program, 75.3% obtained sterile needles from an outreach worker/service, and 64.2% have obtained sterile needles from their dealer or the streets. However, more than one-third (36.3%) indicated they had trouble obtaining enough sterile needles from a service provider to meet their needs. Half (51.0%) indicated that there had been an occasion on which they had wanted to use drugs but didn’t know where to get a sterile needle.
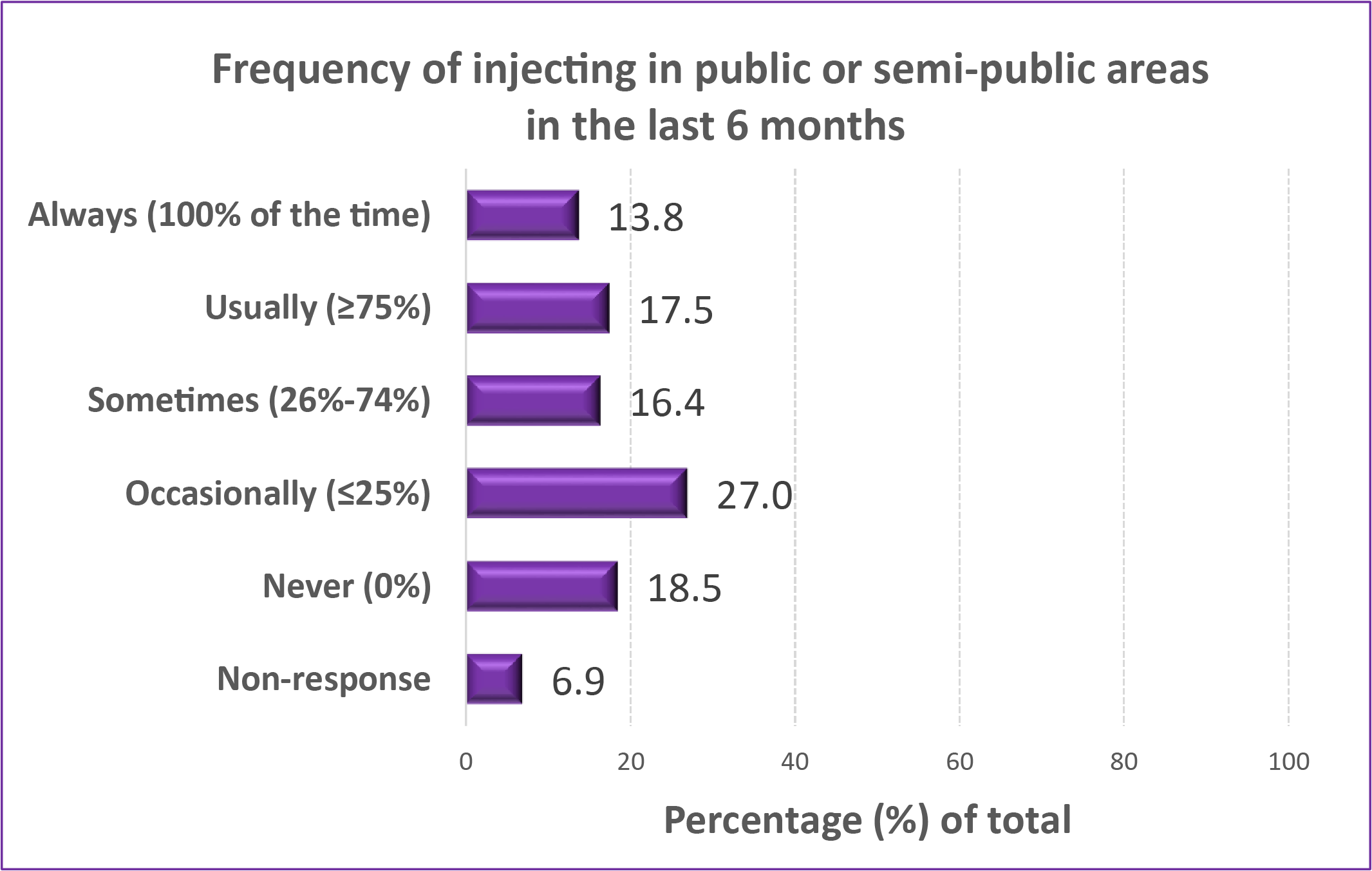
Situations for injecting drugs
Injecting in public may demonstrate that there is a need for designated safe space for injecting94,95,96. Three-quarters (75.0%) of respondents said they had injected drugs in public, with varying frequency, as shown in Figure 3.
Figure 3: Frequency of injecting in public (among those who have ever done so) (%)
In terms of reasons for injecting in public, one-third (35.3%) indicated they inject in public because it was convenient, 25.0% indicated they were too far from home, and 38.0% of PWID respondents reported being homeless in the past 6 months.
Injecting drugs alone poses increased risk of adverse consequences, and injecting with others can mitigate some risk, especially associated with overdose97. The large majority (83.2%) said that they have injected alone, with varying frequency: 18.4% always, 33.5% usually (>75% of time), 21.5% sometimes (26.0-74.0% of time), or 23.4% occasionally (<25% of time). In terms of reasons for injecting in the company of others, half (49.5%) admitted that they have needed help to inject, with varying frequency: 16.0% always, 9.6% usually (>75% of time), 23.4% sometimes (26.0-74.0% of time), or 43.6% occasionally (<25% of time). Other reasons included that 21.6% can’t find a vein on their own, 9.5% don’t know how, and 7.9% prefer someone else to do it.
Infectious disease and medical conditions related to drug use
Drug use, and in particular injecting drug use, carries the risk of infectious disease if equipment is reused or shared98,99,100,101. Screening for disease and referral to treatment are important services that could be provided through SCS. Among the PWID who responded to the survey, more than half (55.5%) had been screened for HIV in the last 6 months; of these, 6 were positive, and of positive cases, 5 are currently accessing treatment. More than half (54.7%) had been screened for hepatitis C in the last 6 months; of these, almost half (45.2%) had contracted hepatitis C, and more than half of those with hepatitis C (55.3%) were not accessing treatment.
PWID also reported other medical conditions that required treatment. These include withdrawal symptoms (20.0%), lung problems (6.8%), abscess (6.3%), injuries (6.3%), depression/psychosis (6.3%), gastrointestinal problems (4.7%), liver problems (4.7%), and blood infection (3.1%).
From the perspective of stakeholders and partners
Drug use: Impact on the health of people who inject drugs
Focus group participants identified an increased incidence of serious medical issues, including large abscesses, blood infections, septicemia, and heart conditions, among people who inject drugs (PWID). The implications for medical and emergency services were also identified, with high rates of individuals accessing ER and hospital services. In addition, PWID may neglect or be unable to make healthy and nutritious food choices if they are spending money on substances and are not in supportive living situations.
Service providers identified a lack of mental illness resources, such as supports for self-care, self-esteem supports, case management, and long wait lists to see psychiatrists. In some cases, it was felt that individuals were using drugs to alleviate mental health symptoms because other treatment options were not available.
In addition, current stigma and oppression, marginalization, and mistreatment towards PWID may lead to them hiding and using alone. Service providers spoke of concurrent mental health issues or underlying trauma, which require supports, including housing. In particular, it was identified that Indigenous people need additional services to address trauma from historical and current racism, colonialism and the “Sixties scoop”. PWID with mental illness are often admitted for psychiatric care due to not complying with community expectations and causing issues in the community.
Drug use: Impact on community, resources, and services
From the perspectives of healthcare providers, emergency departments are the main access point for clients to receive services, but hospitals do not have appropriate outlets to provide a holistic response to the needs of people who inject drugs. Without additional crisis support, or ability to refer individuals to addictions and treatment programs, acute emergency medicine leads to a ‘revolving door,’ with users not receiving support and post-discharge after-care. Users face additional barriers after being discharged from the hospital, particularly with transportation, clothing, and ways of securing food. It was felt that services are not engaging early enough with individuals who inject drugs, given that some clients only connect with institutions when they are at ‘death’s door’.
From the perspectives of law enforcement, drug use creates additional pressures on social services, police, paramedics, and hospitals. Police are being called two to three times a week due to discarded needles and for ambulance calls related to injuries and/or overdoses. There are increased incidences of loitering and property damage. The need for EMS workers and police officers at overdose sites means that they are pulled away from other community needs.
The issues of discarded needles and visible drug use have community implications. People who inject drugs (PWID) are using in unsafe and unsanitary locations downtown. PWID have limited places to go, given that most services, such as shelters, are drug free. Discarded needles in public places such as parks and walkways create risks for community members. Exposing children to drug use and discarded needles creates the potential for injury and the risk of normalizing/ desensitizing injection drug use in public. People appearing intoxicated in public areas creates concern among community members and business owners. Downtown business owners report a loss of business due to visible drug use.
Stakeholders spoke of increased need for security measures in downtown apartment buildings to ensure individuals do not inject in hallways, stairwells and lobbies, particularly during winter months, and said that tenants are afraid of going behind their apartment buildings due to fear that people who inject drugs may become aggressive. It was noted that improper needle disposal may be caused by bail conditions and fear of possession of syringes/drugs. It was noted that the Greater Sudbury community is so vast that it is difficult to measure the amount of need. It is not only the downtown core that is affected. Outlying communities, specifically the “Valley” area (including communities such as Hanmer and Valley East), reportedly have 6-12 police calls a month due to discarded needles.
From the perspective of the Greater Sudbury community
Some respondents to the community survey felt that services would increase the prevalence of drug use and do nothing to decrease the needs; increasing treatment options was considered by some to be the priority. Some observed that SCS align with evidence-based health care policies and best practices, and that these services decrease deaths related to drug use, and reduce opioid overdose and hospital visits. From a public safety perspective, community members spoke of the need to address the opioid epidemic and to prevent used needles from being discarded. Some felt that SCS were long overdue in Sudbury.
“By creating this designated consumption zone, people would be discouraged from consuming drugs in other areas of the city, thereby increasing safety for other citizens.”
Summary: Need
The health harms associated with injection drug use are significant and rising. People who inject drugs in Greater Sudbury continue to experience a variety of social and health risks, despite the existence of some harm reduction supports and services. Drug use creates pressures on social services, police, paramedic, and hospitals. In general, community members expressed the need to further address
drug use and related issues in our community.
Feasibility of supervised consumption services to potential clients, local service providers, and the community
Participants in this study were asked to share their individual perspectives about the conditions under which supervised consumption services (SCS) would be acceptable. Questions related to service provision, site capacity, and utilization were asked to help inform the potential development of SCS for people who inject drugs in Greater Sudbury.
Feasibility of supervised consumption services
From the perspective of people who inject drugs
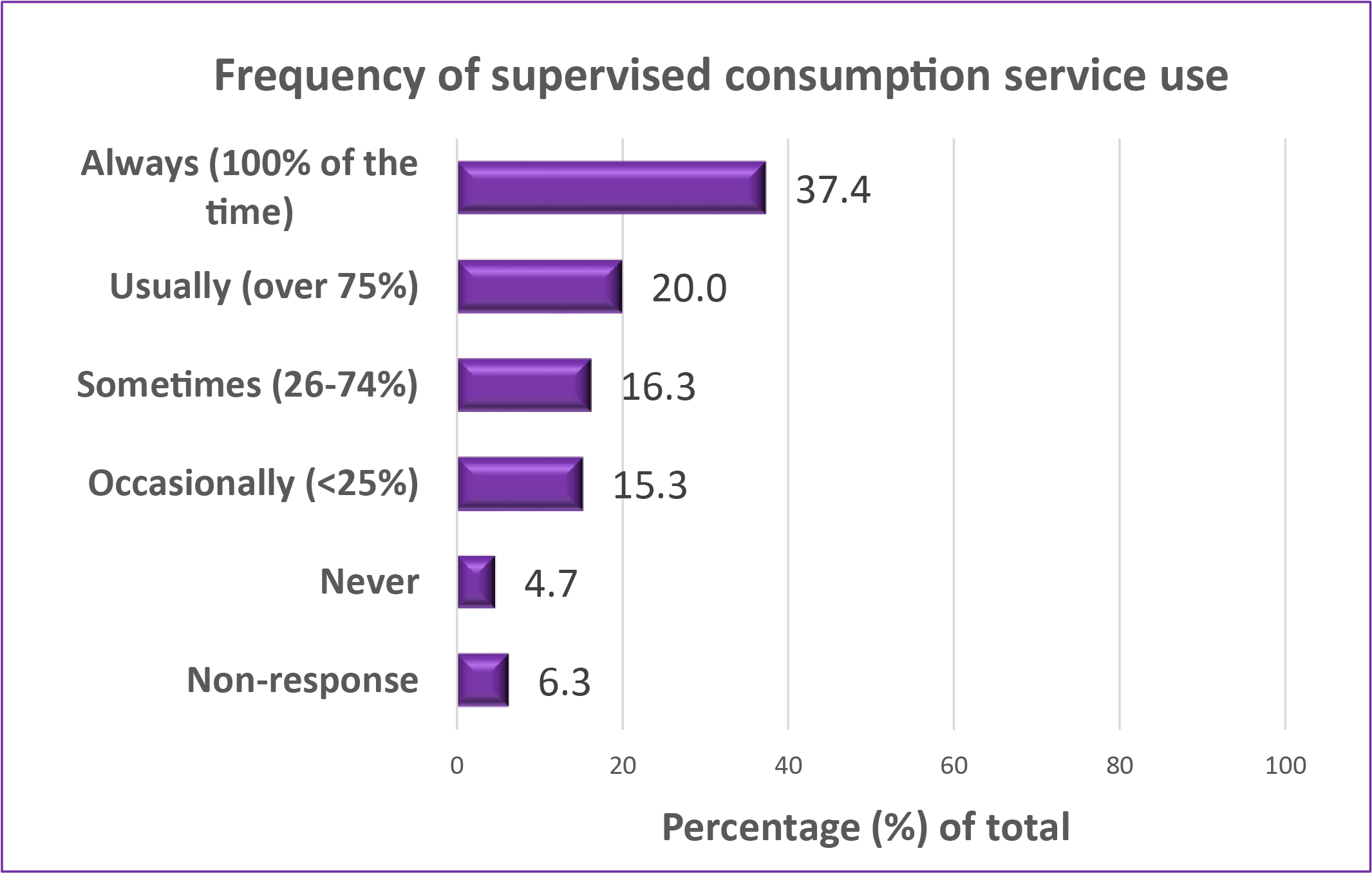
When PWID were initially asked if they had ever heard of SCS prior to the study, only 59.5% indicated that they had. After explaining what SCS entails, participants were asked how often they would use a supervised consumption site. The majority of PWID, 89.0%, indicated that they would be willing to use this type of service, with only 4.7% indicating that they would never use the service, as shown in Figure 4.
Figure 4: Willingness to use SCS (%)
From the perspective of the Greater Sudbury community
Almost two-thirds of community respondents believed that SCS services would be helpful, as shown in Figure 5. Additionally, further analysis demonstrated that the majority of concerns surrounding SCS were largely voiced by the proportion of the community respondents that believed these services would not be helpful.
Figure 5: Would SCS services be helpful? (%)
Service design preferences for supervised consumption services
From the perspective of people who inject drugs
Policies
People who inject drugs were asked to identify their preferences for policies that are commonly implemented in different SCS settings102(percentage indicating the policy would be acceptable is shown):
- injections are supervised by a trained staff member who can respond to overdoses, 89.0%
- 30-minute time limit for injections, 79.5%
- have to hang around for 10 to 15 minutes after injecting so that your health can be monitored, 77.4%
- may have to sit and wait until space is available for you to inject, 69.4%
- have to register each time you use it, 67.4%
- required to show client number, 66.9%
- not allowed to assist each other with injections, 66.3%
- not allowed to share drugs, 59.9%
- not allowed to assist in the preparation of injections, 53.6%
- video surveillance cameras on site to protect users, 50.0%
- required to show government ID, 47.4%
- not allowed to smoke crack or crystal meth, 47.0%
- having to live in the neighbourhood, 44.5%
Accessibility
Walking distance: 83.7% of PWID indicated that they would walk to use SCS, with people generally willing to walk farther distances during the summer than winter months. Of those that responded yes, the greatest proportion (28.3%) indicated that they would walk for up to 20 minutes to access SCS during the summer, 18.9% would walk up to 30 minutes, while many would not walk more than 5 minutes (17.6%) or 10 minutes (18.9%) to access SCS.
Bus access: 72.6% of PWID indicated that they would take a bus to use SCS, with people generally reporting willingness to use bus services equally during the summer than winter months. Of those that responded yes, the greatest proportion (26.8%) indicated that they would take a bus for up to 20 minutes to access SCS during the summer, 26.1% would take a bus up to 30 minutes, 15.2% were willing to take a bus longer than 40 minutes, while 12.3% and 17.4% would not be willing to take a bus longer than 5 minutes or 10 minutes respectively to access SCS.
Hours: 53.9% of PWID indicated that day-time hours (8 a.m. to 4 p.m.) was their first choice for hours of operation, with a second choice of evening hours (44.4%) (4 p.m. to midnight).
Service model and physical arrangement
Peer involvement: 59.5% of PWID believed that peers should be involved with the operation of the SCS.
Space configuration: 41.1% indicated they would prefer private cubicles for use while 23.7% indicated that they would use an open plan with a combination of tables, chairs, and benches.
Drug safety testing: The option of drug safety testing was considered valuable by PWID. The majority of PWID, 91.6%, indicated that they would be willing to wait for results of their drug test before consuming: 14.5% were willing to wait more than 15 minutes; 7.8% were willing to wait between 10 to 15 minutes; 25.3% were willing to wait between 5 to 10 minutes; while 44.0% were only willing to wait up to 5 minutes.
From the perspective of stakeholders and partners
Accessibility
Focus group participants felt that the hours of service for SCS should be determined based on client need, and with awareness of shelter open hours, seasonal patterns, when clients receive their ODSP or OW cheques, access to transportation, and work hours for those employed.
Service model and physical arrangement
Regardless of the specific model, suggested aspects of the approach included:
- creating a welcoming and non-judgmental environment for all clients
- process to encourage regular use on site and not in public
- healing approaches from Elders and traditional healers
- connected to mental health and social services
- creating approaches to ensure that women feel comfortable accessing site, e.g., peer support has been a successful approach at other SCS sites
- collaborative and not siloed
- providing education and understanding about addiction in order to remove stigma and shame
With respect to specific possible models, focus group participants shared the following considerations:
- Fixed SCS: People are already coming downtown; clients build relationships with regular staff.
- Mobile SCS: Greater accessibility, but no regular staff for rapport-building.
- Hybrid (Mobile SCS/fixed location): Flexible, service to city and outlying communities.
Focus group participants also shared ideas on physical space configuration, suggesting that the service be small, with perhaps eight polling booth-style sites or three-sided cubicles. The space might include options for observing, such as mirrors and a raised platform for staff; a quiet room/restful space; and lockers with ‘no questions asked’ storage.
Focus group participants shared the following broad range of potential programs and services that could be a valuable part of SCS, including equipment (e.g. needles), a drop off or exchange needle service, instructions on proper/ safe injection use, testing for drugs so users know what’s in them. Support and referral services suggested included health care and social services, peer support, targeted services (including Indigenous services, with a focus on intergenerational trauma, services for women and for youth), liaison (including OHIP, Ontario Works, food, affordable housing/shelter, mental health/crisis, treatment, withdrawal management/detox). Information for the community was also considered to be an important part of services provided by SCS.
Staffing could include social workers, nurses, nurse practitioners, physicians, clerical staff, security, Indigenous staff, Elders, and traditional healers, peer mentorships and individuals with lived experience, liaison workers, and volunteers. Qualifications of staff should include experience with PWID population; SCS personnel trained in proper safety protocols; and using sensitive language when providing tips on safe injecting practices/habits. Staff training support could include self-regulation and self-care supports for compassion fatigue and burn out; new ways of mitigating risks of addiction; trauma-informed training supports; and tools for building strong relationships with clients.
Leadership and governance
Focus group participants indicated that the development of SCS, and it’s governance structure, should be driven by an advisory committee comprised of participants representing all stakeholders, including individuals with living or lived experience, health and social agencies, and ensuring representation of Indigenous partners. It was suggested that it be run by a social service agency with funding for this purpose and with a link to a health or government organization such as public health, hospital, or addiction service.
Evaluation
Continuous community engagement, ensuring transparency and accountability of meeting milestones, making progress and addressing concerns and needs of the PWID community, will be important elements of success for any potential SCS. The ongoing evaluation of effectiveness of programming will be important.
From the perspective of the Greater Sudbury community
Community survey respondents also had opinions about the service model, and respondents suggested learning from other successful models, such as the Vancouver model, other Canadian cities, and Portugal’s approach for inspiration on decriminalizing.
Community survey respondents were provided with explanations regarding the various types of SCS that exist. Their preferences for type of SCS design were (respondents could choose more than one option):
- 62.4% of community respondents supported an integrated site that offered other services
- 40.2% supported a mobile service that could travel throughout the city
- 26.4% supported a specialized site without other existing health and harm reduction services
- 27.3% were unsure or refused to answer
Similar to stakeholder perspectives, some community survey respondents felt that there should be rigorous evaluation of the services by a third, unbiased party. Some felt that information-sharing would go a long way to sway public opinion, and that Crime Prevention through Environmental Design (CPTED) planning would reduce crime at the site.
A need for attention to onsite security and staff safety training was identified, with differing views on whether or how to incorporate police presence. A range of suggestions included:
- presence of security guards
- passive control of the target community, with firm safety practices, could prove to be effective
- police presence could drive away potential clients of a supervised consumption site, thereby reducing its effectiveness
- police should not be in uniform, but presence would address safety issues
- no police presence: that can be counter-productive
Community survey participants suggested certain rules and processes surrounding SCS, including strict conduct rules that would be police-enforced, rules at the site about selling drugs around the area, needle exchange and disposal rules, prohibitions on usage in the area and having businesses report any other usage in the area. Signs and warnings for the area for pedestrians were also suggested.
“If supervised consumption areas are implemented, any drug use not on the supervising grounds should be met with the fullest extent of the law, not ignored. … People don’t feel safe, and don’t want to be harassed or have their car broken into for trying to support a local business.”
Summary: Feasibility
SCS would be a feasible option for people who inject drugs, and many stakeholders who work in harm reduction and related fields also support SCS. Community members are more mixed in the extent to which SCS are an acceptable option, with 59.8% considering SCS as a helpful option. Specifics about effective design and implementation of SCS were provided, outlining the ways that SCS that could address needs and also be sensitive to community concerns.
How could supervised consumption services be helpful?
The goal of this objective was to identify the extent to which SCS could be helpful, from the perspectives of people who inject drugs, community stakeholders and community members.
From the perspective of people who inject drugs
Among those who would use SCS, the single most important benefit was:
- access to sterile injection equipment (27.5%)
- overdoses can be prevented (20.9%)
- overdoses can be treated (20.3%)
- to inject indoors (11.1%)
Other important benefits were that they would be able to access health professionals; that they would be safe from crime and from being caught by the police; and that they would be able to receive referrals for detox and treatment.
PWID also believed that there would be a number of potential benefits to the community (percentages indicating ‘very likely’ and ‘likely’ responses combined):
- reduction in public injecting (80.5%)
- increase in awareness and knowledge of drug treatment (77.9%)
- reduction in overdoses (77.9%)
- reduction in discarded needles in public (77.4%)
- reduction in reusing needles to inject drugs (76.9%)
- reduction in street violence (59.5%)
- reduction in crime (56.3%)
From the perspective of stakeholders and partners
Stakeholders identified a number of benefits, both for people who inject drugs and for the community. Benefits for people who inject drugs included preventing death due to overdoses, better health outcomes, providing access to other services (information, social worker, nurse, withdraw management, links to education), a strengthened connection and sense of belonging, potential for recovery from addictions for some PWID, and reduction in incarceration of PWID with a focus on harm reduction.
Benefits to the community could include reduction in visible drug use and needle debris, preventing injury from needles (especially for children in public places), containing the issue by having drug use located in one area, improved awareness about addiction and SCS, reduced burden on other services (e.g. hospital beds), and strengthened relationships among community partners to facilitate services.
Stakeholders also spoke of the socioeconomic issues that influence the challenges that clients face. Focus group participants expressed concerns about homelessness and poverty in Greater Sudbury. Homeless clients have no place to return to after treatment, leading to relapse. It was noted that there are high levels of migration and transient individuals coming to Greater Sudbury from other cities.
Other impacts of drug use and addiction include family impacts, given that parents who show visible signs of being injection drug users face increased scrutiny, and mothers may lose custody when accessing treatment programs, detox, and rehab facilities. Stakeholders were concerned about the health impacts on the next generation, such as poor pregnancy outcomes, low gestational age, and babies born with neonatal abstinence syndrome. Family and friends of users are facing emotional impacts of addiction, including guilt, shame, fear, grief, helplessness and concerns about “enabling” people who uses drugs when trying to assist. All of these issues pointed to supports for vulnerable populations that could be provided by supervised consumption services.
Comments from focus groups related to potential benefits included:
“The benefits of having a SCS is that its located in one area, access to other services, so whether it’s drug information or access to other social workers or nurses, or people, I guess ultimately the idea is that if you got a user in front of you, you can try and help them”.
“Injection drug use is a big problem, and we have no outreach to these people. The ED is not the best place because they come in under stress, they are in extremis when they are here…they don’t come in ready to take the next step…or learn about resources. A safe injection site has been shown to help and it might be a better place”.
From the perspective of the Greater Sudbury community
Community respondents were asked to comment on a number of potential and perceived benefits of SCS. Although some respondents said they did not consider SCS to be helpful, and therefore did not answer the questions on benefits, many respondents did identify potential community-related benefits:
- less public drug use on streets or in parks (62.3%)
- less used needles on the streets or in parks (62.3%)
- less risk of injury and death from drug overdose (60.1%)
- help lower the risk of diseases like HIV/AIDS and hepatitis C (59.5%)
- connect people who use drugs or their family members with health, treatment and social services (58.7%)
- increase community safety (53.0%)
- less work for ambulance and police services (45.2%)
Similar suggestions of possible services were provided, although the focus among community survey respondents emphasized referrals and availability of treatment and rehab options. Other services suggested included needle exchange, drug testing, and safe space to be after injecting. Supports such as health care, housing, showers and food, and a generally non-judgemental approach were also mentioned.
Summary: Helpful
Aspects of SCS that could be helpful were identified, including access to sterile needles, preventing and treating overdoses, connecting people who use drugs with education, treatment, and support options, less public drug use and fewer discarded needles in public spaces, and reducing the burden on ambulance and police services. Some community residents do not consider that SCS would be a helpful addition to services in Sudbury, and suggest that resources either not go to supporting people who inject drugs, or that resources go toward treatment and abstinence options.
Concerns associated with supervised consumption services, and mitigation strategies
The goal of this objective was to identify concerns, challenges, and/or barriers that might be associated with SCS in Greater Sudbury and identify potential mitigation strategies to address them.
From the perspective of people who inject drugs
Approximately one-third of respondents to the PWID survey (35.8%) were not familiar with the supervised consumption service terminology. When the concept was explained, 89.0% of PWID indicated that they would make use of SCS. However, for those who responded that they would not use, or may not use these services frequently, the following themes were noted as potential concerns, challenges, and barriers:
- Anonymity: A number of PWID expressed that they did not want to be seen accessing the services, or let others know they use illicit drugs, and had fears that it would be difficult to access these services confidentially.
- Fear of police: A number of PWID expressed that they were concerned that police would target the area and that accessing the SCS may increase their chances of being arrested.
- Self-sufficient: A number of PWID indicated they had a safe place to inject and were able to obtain needles and equipment through other services, that there would be too many rules and regulations, and that it likely wouldn’t be convenient for them (neither the physical location nor the time required to access and use the services).
Additionally, PWID acknowledged that there would be increased traffic to the area surrounding the SCS. Specifically, 70.0% of PWID believed that they and others would visit the area, and 48.4% indicated that PWID may choose to move into the area. Half of the PWID respondents also believed that it was likely that drug dealers would be attracted to the area.
From the perspective of stakeholders and partners
Stakeholders identified a number of concerns for people who inject drugs, about negative community feedback, lack of awareness, concerns about funding and infrastructure, and concerns about implementation of SCS.
Concerns for PWID
There was a concern that SCS would not be enough to meet all the needs of PWID, allowing them to move from SCS to potential recovery and follow-up. The specific needs of youth were also identified. There was a concern for discretion and anonymity for PWID within and around SCS, and concern regarding stigma and discrimination by service providers.
Concerns about community
Business owners near any possible SCS site fear a loss of customers/business, and individuals who live, work or transit near a SCS site have concerns for safety, fear of increase in crime and violence, police and EMS. They noted that if a fixed SCS is selected, there would need to be a way to mitigate the impact on the surrounding area.
It was felt by some focus group participants that these concerns are due to lack of knowledge about the benefits and effectiveness of SCS, and lack of understanding about mental health/illness and link to addiction, and that increased awareness could mitigate some of the concern.
Mitigation strategies
Careful planning of SCS would include awareness and education, including related to the social cost of the status quo (for people who use drugs and for the community) and the benefits of SCS for better health outcomes. Ideas to mitigate concerns about implementing SCS services included careful planning and recruitment of the “right” staff; adequate and proper training for staff and good supports for peer support workers; establishing rules that are understood by all; promoting placement opportunities (e.g. physicians, nurses); and building relationships with PWID to ensure they feel respected and supported and continue to use the SCS.
From the perspective of the Greater Sudbury community
As previously noted, 59.8% believed that SCS would be helpful in Sudbury and 33.6% did not believe such services would be helpful. Almost half (46.6%) of the community respondents indicated that they had concerns about SCS, while 42.8% had none, 6.3% were neutral, and 2.5% were unsure. Although concerns were raised by fewer than half of the survey respondents, meaning that these concerns are not universal, these perceptions would need to be addressed if SCS are established in Greater Sudbury.
Concerns
Approximately one-third of respondents had concerns that SCS could lead to more drug selling or trafficking in the area, more people who use drugs in the area, more drug use, concerns about property values, community reputation, impact on business, and personal safety.
In their comments, some community survey respondents reflected concern for PWID, including safety concerns for PWID, impacts by those opposed to the site, and lack of available supports and services. Respondents also expressed safety concerns for staff and for community, including potentially sending a message to youth that drug use is condoned. Some community members said that SCS were an inappropriate use of tax dollars, and some made the comparison that it was unfair for diabetics who have to pay for their needles. Some said that increased enforcement and tougher penalties would be their preferred approach, and that SCS simply encouraged more drug use and would result in a clustering of drug dealers, an increase in criminal activity, and would result in an increase in overdoses. Some doubted that PWID would actually travel to the services, and that the current problems would not be addressed through SCS.
Some felt that increasing treatment options should be the priority, with more rehabilitation and detox centres, more counselling for addiction/mental health issues, and referrals to other treatment centres. The long-term sustainability and coordination of services was considered to be important.
Mitigation strategies
Community residents were asked to provide feedback on some common mitigation strategies. Responses included public awareness about the goals of SCS, having a community group to work on issues about SCS, evaluating the services, and increased lighting and police presence in the area. A coordinated approach involving all social services, including attention to needle exchange and disposal were other suggestions of ways to address potential concerns.
Summary: Concerns and mitigation
As with any new approach to an issue, there are concerns expressed by all those affected. PWID have concerns about maintaining anonymity and being arrested around a SCS site. Stakeholders felt that SCS would need to be carefully designed and resourced if they are to be successful. Stakeholders and community members had cautions related to neighbourhood safety and an increase in drug use and trafficking in a particular area.
Some community members supported SCS despite having some concerns, and some did not feel that they could support SCS. Many stakeholders were aware of SCS in other communities and felt that Greater Sudbury could learn from these examples to mitigate potential problems and develop effective SCS. Mitigation strategies included sharing information about SCS with community members; evaluating and making changes to remediate any issues; increasing safety in the area; and having a community advisory group to receive feedback and address concerns.
Determine how supervised consumption services could be integrated with existing harm reduction services
The goal of this objective was to determine how SCS could be integrated with existing harm reduction services in Greater Sudbury.
As previously noted, PWID already use many existing harm reduction services, including needle exchange, naloxone kits, blood testing, detox, and drug treatment.
From the perspective of stakeholders and partners
Stakeholders noted that there is good collaboration and communication between organizations in the city around drug use, and that there is support for a systems approach to SCS delivery. Focus group participants felt it was important to build on existing harm reduction programs in Greater Sudbury. Organizations who offer such programs were identified as having the appropriate approach/model to support the needs of those who would use SCS, as well as the needs of the larger community. Integration and linking of services did not necessarily translate to co-location of all services, recognizing that established services fill a need and that there could be value in maintaining some dispersion of services.
Many ideas were advanced about how SCS could work in partnership and coordination with other services. One possible model was to have integrated SCS services attached to a service already being used by PWID (e.g., methadone clinic, public health, hospital, clinic, CMHA low barrier shelter). Another concept was for SCS to provide a hub of harm reduction services from organizations and programs such as Monarch Recovery, Réseau ACCESS Network, Crisis Intervention Services, Corner Clinic and needle exchange program that would align services with the needs of the clients.
Harm reduction services that can be delivered in collaboration with local organizations include naloxone training, case management, counselling services, drug testing, and referrals to medical care and housing services. Building collaborative partnerships with harm reduction services may help tackle the reason why there is improper needle disposal in the community. Participants shared that
partnering with outreach workers from Sudbury Action Centre for Youth (SACY) have been shown to be successful due to their strong relationships with the PWID community and their experience with the needle exchange program.
Integrating Indigenous organizations that provide harm reduction services was also advanced as a priority. Participants stated that incorporating Indigenous healing approaches such as traditional smudging, ceremonies and a designated healing room would be beneficial for clients accessing the SCS. Indigenous programming can align with current services provided by local Indigenous organizations such as N’Swakamok Native Friendship Centre, Shkagamik’kwe Health Centre, and Aboriginal Peoples Alliance of Northern Ontario (APANO). Indigenous services can be delivered by Elders, traditional healers and Indigenous navigators with a focus on intergenerational trauma and the impacts of historical colonization and assimilation experienced by Indigenous communities.
Providing resources and maintaining partnerships to attain affordable housing for clients of SCS was advanced as a priority. The Canadian Mental Health Association (CMHA) Sudbury/Manitoulin’s low barrier shelter was noted by participants as an example of a service that can align closely with the housing component of the SCS. The Off the Streets emergency low-barrier shelter provides a facility for the chronically homeless who experience substance abuse and mental illness challenges. The program is also accompanied by the Harm Reduction Home (HRH), a managed alcohol program for individuals who struggle with severe alcohol dependence.
Integrating mental health and psychiatric services to reduce waitlists to receive care was another priority. It was expressed that utilizing a peer support navigator from Northern Initiative for Social Action (NISA) in the hospital setting would address clients concerns with mental health and addiction challenges. Focus group participants stated that clients may be more inclined to disclose information to an individual with lived experience. A centralized intake tool was suggested, to enforce collaboration between health care and social service agencies in the community. It was noted that there would be ongoing need for financial resources, with budget increases for growing need, staffing, and supplies.
With respect to service integration, it was noted that Health Sciences North’s Rapid Access Addiction Medicine (RAAM Clinic), or other addiction treatment services, should not co-exist within the same site. Allowing individuals to actively consume substances in the same environment as those seeking treatment options may be a trigger for some individuals.
From the perspective of the Greater Sudbury community
As noted previously, 62.4% of survey respondents supported an integrated site that also offers other services (see Figure 6).
Figure 6: Preferred service-model design of SCS (%)
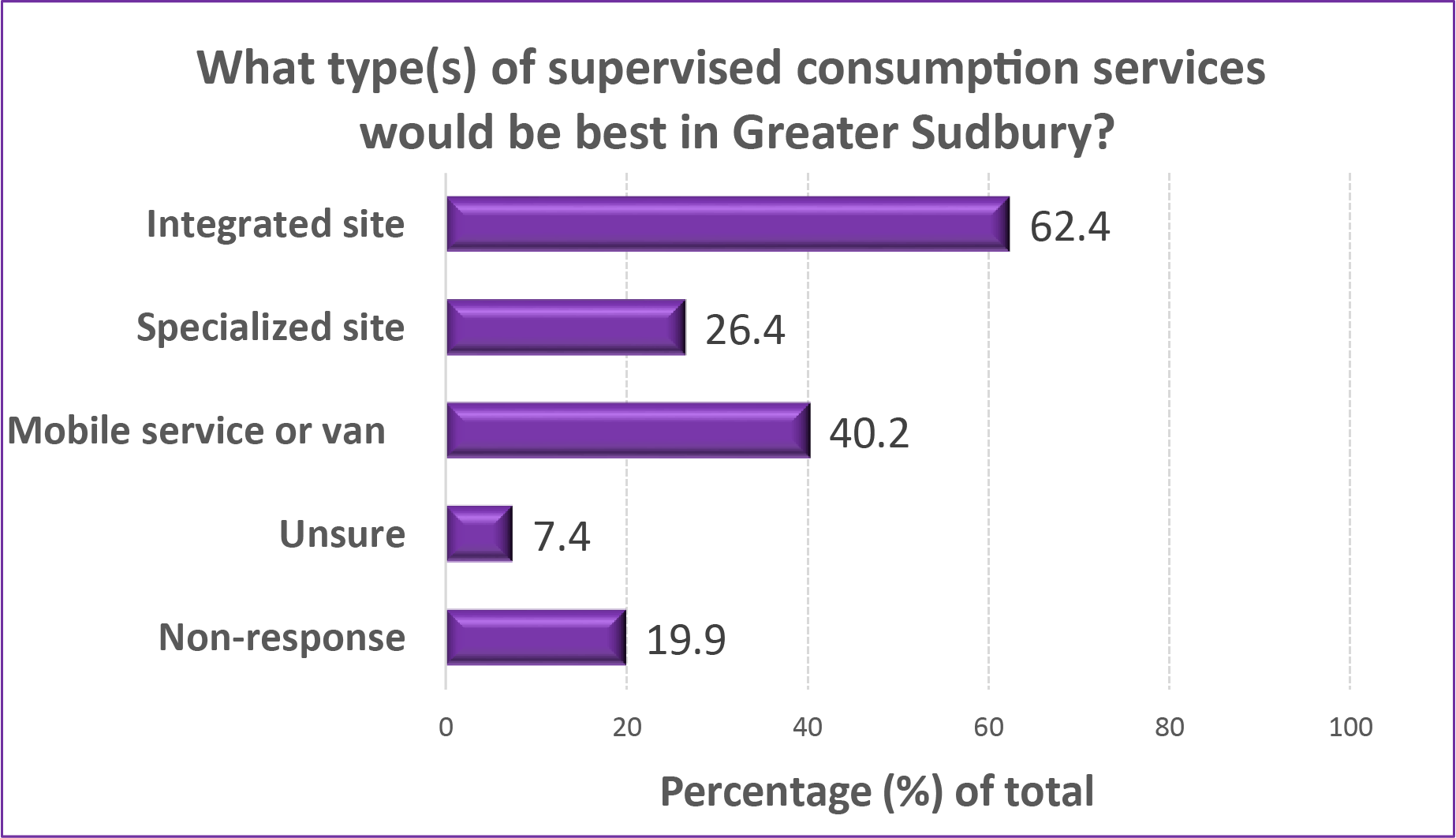
Summary: Integration of services
Stakeholders felt that it would be valuable to build on existing good collaboration and communication between organizations in the city related to harm reduction leading to a stronger, coordinated system that would include SCS. Additional consultation would be required to determine all partners who want/need to be involved to make this programming successful. Among those who responded, many community members supported a SCS site that also offers other services and is integrated with existing programs.
Potential locations for supervised consumption services
The goal of this objective was to determine potential locations for SCS.
From the perspective of people who inject drugs
The preference by the people who inject drugs participants was for the SCS to be located at a stand-alone location (72.6%), while there was some support to have it co-located in a community health center (61.6%), walk-in clinic (51.1%), hospital (40.0%), social service agency (38.9%) or family doctor’s clinic (37.9%).
PWID were shown a detailed map of the city. The majority of PWID (65.8%) indicated their preferred location for SCS was the central region of ‘Sudbury,’ which included the following neighbourhoods: Donovan, Downtown, Flour Mill, Kingsmount-Bell Park, Minnow Lake, and the West End. Additionally, some PWID suggested New Sudbury (9.5%) and outlying areas such as Azilda, Coniston, or Garson (12 different suggestions, cumulatively 14.2%) were also suggested.
From the perspective of stakeholders and partners
In general, focus group participants suggested that SCS should be located in a centralized location downtown. The majority of health care and social services are located in the downtown core: e.g. Réseau ACCESS Network, The Mission (Samaritan Centre), shelters, and there would be close proximity to food banks, nurse practitioners, ODSP/OW office, Public Health Sudbury & Districts (Rainbow Centre), needle exchange, and others. The needs of individuals who live on the outskirts of Sudbury would also have to be considered.
Focus group members also brought forward considerations of safety and comfort for individuals in the larger community and for people who inject drugs. Considerations for location would be that the site is convenient for clients, in terms of transit access, walking access, near drug activity, and where people socially congregate. Other ways of determining location would be to determine hot spots throughout the community that have higher rates of need e.g. overdoses, discarded needles, infectious diseases, etc.
From the perspective of the Greater Sudbury community
Almost 1400 community respondents offered suggestions regarding the potential location for SCS in Greater Sudbury. Overwhelmingly respondents suggested ‘downtown’ Greater Sudbury, with many providing specific street locations or existing agencies where these services could be co-located, such as the Mission or the low barrier shelter. Additionally, some community respondents included adjacent downtown neighbourhoods, specifically the ‘Donovan’ and ‘Flour Mill’ areas of the city. Many respondents also suggested that the location should be chosen based on where the need for the services is highest, where drug use is already happening, or in a location that is easy to get to. Some respondents suggested SCS should not be located downtown because other services were already there but rather these services should be available elsewhere in the city as well. Community respondents felt that the SCS should not be in close proximity to schools or other community locations occupied by children. Some community respondents, 40.2%, felt that a mobile van would also be a possible solution.
Comments from community survey respondents include that the choice of a site is important and would have an impact on the image of downtown areas as well as an impact on children, families, and community members. If a single site is selected, this could lead to a concentration of drug users in one neighbourhood, which could potentially negatively impact that specific area, increase crime, violence and danger in that area, and have a negative impact on business. A variety of perspectives were advanced:
“No one will want to visit/shop anywhere around the location of the safe injection site. The location could kill potential business around it.”
“Location choice should be data-driven to reflect consumption levels and need for services. If there is one placed somewhere in Sudbury proper, there should be additional locations placed in outlying communities also as required. A threshold limit for observed level of injection drug use should be established and any area with sufficiently high consumption should have a safe injection site.”
“Downtown. As someone that works downtown this is definitely needed. If it offered more services as well, it would be used. There is a gap in what is available for the populations most vulnerable.”
“Industrial section, where there are no children or visitors. NOT the downtown core, and NOT near people’s houses.”
“Not downtown. We can’t encourage business that will pay taxes that support supervised sites if people are roaming streets day and night. Use mobile sites all around the region where people can live and find family support.”
“Perhaps downtown near shelters. If those with addictions have to struggle to find transportation to travel to a location, they may not make use of the consumption site.”
“One in the neighbourhood around the bridge of nations and one around the west end. I think experts need to look for where use already happens. Main thing is to have it in range of one bus from downtown terminal.”
“Permanent location should be in the epicentre of where most users are. Mobile one could travel to other most used areas as well as in the outskirts. i.e., Chelmsford, Wahnapitae, etc.”
Summary: Potential location
If SCS are established in Greater Sudbury, basing decisions about location on data was felt to be the best course of action, considering where users currently reside and congregate and where other services are available, and also keeping community safety and comfort in mind. Among those who would consider the option of SCS, a downtown location and/or a mobile service were supported by community members.
Concluding remarks
The overall purpose of this study was to determine the need for and the feasibility of implementing supervised consumption services in the City of Greater Sudbury, from the perspective of all community stakeholders.
This study identifies significant and growing health impacts associated with injection drug use in Greater Sudbury that would be mitigated by SCS.
In order to be feasible for the City of Greater Sudbury, SCS would need to address a number of concerns raised in this study.
Potential clients would use SCS, if available. Among community survey respondents, 59.8% believed that these services would be helpful in Greater Sudbury and 33.6% of respondents did not believe these types of services would be helpful.
Potential benefits identified by community respondents include less public drug use on streets or in parks, fewer used needles on the streets or in parks, and less risk of injury and death from drug overdose. Concerns expressed in the community survey were related to neighbourhood safety, an increase in crime and drug use, and more drug dealers targeting the area.
Concerns could be addressed through strategies such as having a community group to work on issues about SCS, effectively communicating information about the goals and benefits of SCS, and evaluating the services.
If SCS are considered in Greater Sudbury, a location must be carefully chosen. The most common suggestion was a centralized location in the downtown core, in proximity to, and integrated with, existing harm reduction services and the majority of health care and social services.
Endnotes
1 British Columbia Centre on Substance Use (BCCSU). (2017). Supervised Consumption Services: Operational Guidance. Retrieved from https://www.bccsu.ca/ wp-content/uploads/2017/07/BC-SCS-Operational-Guidance.pdf
2 British Columbia Centre on Substance Use (BCCSU). (2017). Supervised Consumption Services: Operational Guidance. Retrieved from https://www.bccsu.ca/ wp-content/uploads/2017/07/BC-SCS-Operational-Guidance.pdf
3 British Columbia Centre on Substance Use (BCCSU). (2017). Supervised Consumption Services: Operational Guidance. Retrieved from https://www.bccsu.ca/wp-content/uploads/2017/07/BC-SCS-Operational-Guidance.pdf
4 Public Health Sudbury & Districts. (2015). Community drug strategy for the City of Greater Sudbury: A Call To Action. Retrieved from https://www.phsd.ca/wp-content/uploads/2018/01/NewDrugStrategy_Feb-2016-3.pdf
5 Public Health Sudbury & Districts. (2015). Community drug strategy for the City of Greater Sudbury: A Call To Action. Retrieved from https://www.phsd.ca/wp-content/uploads/2018/01/NewDrugStrategy_Feb-2016-3.pdf
6 British Columbia Centre on Substance Use (BCCSU). (2017). Supervised Consumption Services: Operational Guidance. Retrieved from https://www.bccsu.ca/wp-content/uploads/2017/07/BC-SCS-Operational-Guidance.pdf
7 Poschadel, S., Höger, R., Schnitzler, J., & Schreckenberg, D. (2003). Evaluation of the work of drug consumption rooms in the Federal Republic of Germany. Abridged version of the final report on behalf of the Federal Ministry of Health.
8 Potier, C., Laprévote, V., Dubois-Arber, F., Cottencin, O., & Rolland, B. (2014). Supervised Consumption Services: what has been demonstrated? A systematic literature review. Drug and Alcohol Dependence, 145, 48–68. https://doi.org/10.1016/j.drugalcdep.2014.10.012
9 Marshall, B. D. L., Milloy, M. J., Wood, E., Montaner, J. S., & Kerr, T. (2011). Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: a retrospective population-based study. The Lancet, 377(9775), 1429-1437. https://doi.org/10.1016/S0140-6736(10)62353-7
10 Wood, E., Kerr, T., Small, W., Li, K., Marsh, D. C., Montaner, J. S. G., & Tyndall, M. W. (2004). Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Canadian Medical Association Journal, 171(7), 731–734.
11 Wood, E., Kerr, T., Small, W., Li, K., Marsh, D. C., Montaner, J. S. G., & Tyndall, M. W. (2004). Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Canadian Medical Association Journal, 171(7), 731–734.
12 Kerr, T., Tyndall, M., Li, K., Montaner, J., & Wood, E. (2005). Safer injection facility use and syringe sharing in injection drug users. The Lancet, 366(9482), 316–318. Retrieved from https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(05)66475-6/fulltext
13 Bayoumi, A. M., & Zaric, G. S. (2008). The cost-effectiveness of Vancouver’s supervised injection facility. Canadian Medical Association Journal, 179(11), 1143–1151. https://doi.org/10.1503/cmaj.080808
14 Pinkerton, S. D. (2011). How many HIV infections are prevented by Vancouver Canada’s supervised injection facility? International Journal of Drug Policy, 22(3), 179–183. https://doi.org/10.1016/j.drugpo.2011.03.003
15 Stoltz, J.-A., Wood, E., Small, W., Li, K., Tyndall, M., Montaner, J., & Kerr, T. (2007). Changes in injecting practices associated with the use of a medically supervised safer injection facility. Journal of Public Health (Oxford, England), 29(1), 35–39. https://doi.org/10.1093/pubmed/fdl090
16 Wood, R. A., Wood, E., Lai, C., Tyndall, M. W., Montaner, J. S. G., & Kerr, T. (2008). Nurse-delivered safer injection education among a cohort of injection drug users: evidence from the evaluation of Vancouver’s supervised injection facility. The International Journal on Drug Policy, 19(3), 183–188.
17 Fast, D., Small, W., Wood, E., & Kerr, T. (2008). The perspectives of injection drug users regarding safer injecting education delivered through a supervised injecting facility. Harm Reduction Journal, 5, 32.
18 Marshall, B. D. L., Wood, E., Zhang, R., Tyndall, M. W., Montaner, J. S. G., & Kerr, T. (2009). Condom use among injection drug users accessing a supervised injecting facility. Sexually Transmitted Infections, 85(2), 121–126. https://doi.org/10.1136/ sti.2008.03252
19 Potier, C., Laprévote, V., Dubois-Arber, F., Cottencin, O., & Rolland, B. (2014). Supervised Consumption Services: what has been demonstrated? A systematic literature review. Drug and Alcohol Dependence, 145, 48–68. https://doi.org/10.1016/j. drugalcdep.2014.10.012
20 Wood, E., Kerr, T., Small, W., Li, K., Marsh, D. C., Montaner, J. S. G., & Tyndall, M. W. (2004). Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Canadian Medical Association Journal, 171(7), 731–734.
21 Bayoumi, A. M., & Zaric, G. S. (2008). The cost-effectiveness of Vancouver’s supervised injection facility. Canadian Medical Association Journal, 179(11), 1143–1151. https://doi.org/10.1503/cmaj.080808
22 Lloyd-Smith, E., Wood, E., Zhang, R., Tyndall, M. W., Montaner, J. S., & Kerr, T. (2009). Determinants of cutaneous injection-related infection care at a supervised injecting facility. Annals of Epidemiology, 19(6),404–409. https://doi.org/10.1016/j.annepidem.2009.03.007
23 Wood, E., Tyndall, M. W., Zhang, R., Montaner, J. S. G., & Kerr, T. (2007). Rate of detoxification service use and its impact among a cohort of supervised injecting facility users. Addiction (Abingdon, England), 102(6), 916–919. https://doi.org/10.1111/j.1360-0443.2007.01818.x
24 Kimber, J., Mattick, R. P., Kaldor, J., van Beek, I., Gilmour, S., & Rance, J. A. (2008). Process and predictors of drug treatment referral and referral uptake at the Sydney Medically Supervised Injecting Centre. Drug and Alcohol Review, 27(6), 602–612. Retrieved from https://doi.org/10.1080/09595230801995668
25 Wood, E., Tyndall, M. W., Montaner, J. S., & Kerr, T. (2006b). Summary of findings from the evaluation of a pilot medically supervised safer injecting facility. Canadian Medical Association Journal, 175(11), 1399–1404. https://doi.org/10.1503/ cmaj.060863
26 DeBeck, K., Kerr, T., Bird, L., Zhang, R., Marsh, D., Tyndall, M., … Wood, E. (2011). Injection drug use cessation and use of North America’s first medically supervised safer injecting facility. Drug and Alcohol Dependence, 113(2-3), 172–176.Retrieved from https://doi.org/10.1016/j.drugalcdep.2010.07.023
27 Krusi, A., Small, W., Wood, E. & Kerr, T. (2009). An integrated supervised injecting program within a care facility for HIV-positive individuals: a qualitative evaluation. AIDS Care, 21:5, 638-644.
28 Wood, E., Tyndall, M. W., Zhang, R., Montaner, J. S. G., & Kerr, T. (2007). Rate of detoxification service use and its impact among a cohort of supervised injecting facility users. Addiction (Abingdon, England), 102(6), 916–919. https://doi.org/10.1111/j.1360-0443.2007.01818.x
29 Kimber, J., Mattick, R. P., Kaldor, J., van Beek, I., Gilmour, S., & Rance, J. A. (2008). Process and predictors of drug treatment referral and referral uptake at the Sydney Medically Supervised Injecting Centre. Drug and Alcohol Review, 27(6), 602–612. Retrieved from https://doi.org/10.1080/09595230801995668
30 DeBeck, K., Kerr, T., Bird, L., Zhang, R., Marsh, D., Tyndall, M., … Wood, E. (2011). Injection drug use cessation and use of North America’s first medically supervised safer injecting facility. Drug and Alcohol Dependence, 113(2-3), 172–176.Retrieved from https://doi.org/10.1016/j.drugalcdep.2010.07.023
31 Milloy, M.-J. S., Kerr, T., Zhang, R., Tyndall, M., Montaner, J., & Wood, E. (2009). Inability to access addiction treatment and risk of HIV infection among injection drug users recruited from a supervised injection facility. Journal of Public Health, 32(3), 342-349. https://doi.org/10.1093/pubmed/fdp089
32 Wood, E., Tyndall, M. W., Lai, C., Montaner, J. S., & Kerr, T. (2006a). Impact of a medically supervised safer injecting facility on drug dealing and other drug-related crime. Substance Abuse Treatment, Prevention, and Policy, 1, 13. https://doi. org/10.1186/1747-597X-1-13
33 Salmon, A. M., van Beek, I., Amin, J., Kaldor, J., & Maher, L. (2010). The impact of a supervised injecting facility on ambulance call-outs in Sydney, Australia. Addiction (Abingdon, England), 105(4), 676–683. https://doi.org/10.1111/j.1360-0443.2009.02837.x
34 Wood, E., Kerr, T., Small, W., Li, K., Marsh, D. C., Montaner, J. S. G., & Tyndall, M. W. (2004). Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Canadian Medical Association Journal, 171(7), 731–734.
35 Stoltz, J.-A., Wood, E., Small, W., Li, K., Tyndall, M., Montaner, J., & Kerr, T. (2007). Changes in injecting practices associated with the use of a medically supervised safer injection facility. Journal of Public Health (Oxford, England), 29(1), 35–39. https://doi.org/10.1093/pubmed/fdl090
36 Wood, E., Kerr, T., Small, W., Li, K., Marsh, D. C., Montaner, J. S. G., & Tyndall, M. W. (2004). Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Canadian Medical Association Journal, 171(7), 731–734.
37 Stoltz, J.-A., Wood, E., Small, W., Li, K., Tyndall, M., Montaner, J., & Kerr, T. (2007). Changes in injecting practices associated with the use of a medically supervised safer injection facility. Journal of Public Health (Oxford, England), 29(1), 35–39. https://doi.org/10.1093/pubmed/fdl090
38 Fast, D., Small, W., Wood, E., & Kerr, T. (2008). The perspectives of injection drug users regarding safer injecting education delivered through a supervised injecting facility. Harm Reduction Journal, 5, 32.
39 Potier, C., Laprévote, V., Dubois-Arber, F., Cottencin, O., & Rolland, B. (2014). Supervised Consumption Services: what has been demonstrated? A systematic literature review. Drug and Alcohol Dependence, 145, 48–68. https://doi.org/10.1016/j.drugalcdep.2014.10.012
40 Wood, E., Tyndall, M. W., Qui, Z., Zhang, R., Montaner, J. S. G., Kerr, T. (2006). Service uptake and characteristics of injection drug users utilizing North America’s first medically supervised safer injecting facility. American Journal of Public Health, 96(5): 770-773.
41 Kerr, T., Tyndall, M. W., Zhang, R., Lai, C., Montaner, J. S. G., & Wood, E. (2007). Circumstances of first injection among illicit drug users accessing a medically supervised safer injection facility. American Journal of Public Health, 97(7), 1228– 1230. https://doi.org/10.2105/AJPH.2006.086256
42 Bayoumi, A. M., & Zaric, G. S. (2008). The cost-effectiveness of Vancouver’s supervised injection facility. Canadian Medical Association Journal, 179(11), 1143–1151. https://doi.org/10.1503/cmaj.080808
43 Pinkerton, S. D. (2011). How many HIV infections are prevented by Vancouver Canada’s supervised injection facility? International Journal of Drug Policy, 22(3), 179–183. https://doi.org/10.1016/j.drugpo.2011.03.003
44 Ontario Integrated Supervised Injection Services Feasibility Study (OiSiS). (2017). Study Report: Thunder Bay, ON. Retrieved from https://www.google.com/search?q=thunder+bay+injection+site+report&rlz=1C1GCEU_enCA827CA827&oq=thunder+bay+injection+site+report&aqs=chrome..69i57j69i59.5364j0j8&sourceid=chrome&ie=UTF-8
45 Ontario Integrated Supervised Injection Services Feasibility Study (OiSiS). (2017). Study Report: London, ON. Retrieved from https://www.waterlooregiondrugstrategy.ca/en/data-and-research/studies-reviews-and-reports.aspx
46 Region of Waterloo Public Health and Emergency Services. (2018). Waterloo Region Supervised Injection Services Feasibility Study. Retrieved from https://www.waterlooregiondrugstrategy.ca/en/data-and-research/studies-reviews-and-reports.%20aspx
47 City of Greater Sudbury. (2020). Location. Retrieved from: https://www.greatersudbury.ca/live/about-greater-sudbury/location/
48 Statistics Canada. (2019). Census Profile, 2016 Census. Retrieved from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=CD&Code1=3553&Geo2=PR&Code2=47&SearchText=greater%20sudbury&SearchType=Begins&SearchPR=01&B1=All&TABID=1&type=0
49 Statistics Canada. (2019). Census Profile, 2016 Census. Retrieved from: https:// www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page. cfm?Lang=E&Geo1=CD&Code1=3553&Geo2=PR&Code2=47&SearchText=greater%20sudbury&SearchType=Begins&SearchPR=01&B1=All&TABID=1&type=0
50 Statistics Canada. (2019). Census Profile, 2016 Census. Retrieved from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=CD&Code1=3553&Geo2=PR&Code2=47&SearchText=greater%20sudbury&SearchType=Begins&SearchPR=01&B1=All&TABID=1&type=0
51 Statistics Canada. (2019). Census Profile, 2016 Census. Retrieved from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=CD&Code1=3553&Geo2=PR&Code2=47&SearchText=greater%20sudbury&SearchType=Begins&SearchPR=01&B1=All&TABID=1&type=0
52 Statistics Canada. (2019). Census Profile, 2016 Census. Retrieved from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=CD&Code1=3553&Geo2=PR&Code2=47&SearchText=greater%20sudbury&SearchType=Begins&SearchPR=01&B1=All&TABID=1&type=0
53 Kauppi, C., Pallard, H., Faries, E., Montgomery, P., Hankard, M. (2018). Homelessness in the City of Greater Sudbury: 2018 Enumeration. June 2018. Report prepared for the City of Greater Sudbury. Centre for Research in Social Justice and Policy, Laurentian University, Sudbury, Ontario. Retrieved from https://www.greatersudbury.ca/live/housing-landing-page/housing-services/homelessness-initiatives/homelessness-count-conducted-by-laurentian-university-in-march-2018/
54 Kauppi, C., Pallard, H., Faries, E., Montgomery, P., Hankard, M. (2018). Homelessness in the City of Greater Sudbury: 2018 Enumeration. June 2018. Report prepared for the City of Greater Sudbury. Centre for Research in Social Justice and Policy, Laurentian University, Sudbury, Ontario. Retrieved from https://www.greatersudbury.ca/live/housing-landing-page/housing-services/homelessness-initiatives/homelessness-count-conducted-by-laurentian-university-in-march-2018/
55 City of Greater Sudbury. (2018). Demographic Data in the City of Greater Sudbury. Retrieved from https://www.arcgis.com/apps/MapSeries/index.html?appid=2624ebe80fcc435d993f446d66920f51
56 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/point-harm-reduction-supplies-services
57 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/point-harm-reduction-supplies-services
58 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/point-harm-reduction-supplies-services
59 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/point-harm-reduction-supplies-services
60 Sudbury Temporary Overdose Prevention Society (STOP). (2019). Demographic and client utilization rates. [Internal raw data].
61 Sudbury Temporary Overdose Prevention Society (STOP). (2019). Demographic and client utilization rates. [Internal raw data].
62 Sudbury Temporary Overdose Prevention Society (STOP). (2019). Demographic and client utilization rates. [Internal raw data].
63 Sudbury Action Centre for Youth. (2020). About Us. Retrieved from: http://www.sacy.ca/home/about/
64 Sudbury Action Centre for Youth. (2020). About Us. Retrieved from: http://www.sacy.ca/home/about/
65 Public Health Sudbury & Districts. (2018). Community Drug Strategy for the City of Greater Sudbury: A Call to Action [Updated]. Retrieved from https://www.phsd. ca/wp content/uploads/2018/01/ExecutiveSummary_Feb2015.pdf
66 Public Health Sudbury & Districts. (2018). Community Drug Strategy for the City of Greater Sudbury: A Call to Action [Updated]. Retrieved from https://www.phsd.ca/wpcontent/uploads/2018/01/ExecutiveSummary_Feb2015.pdf
67 Greater Sudbury Police Services. (2019). Impacts of increased foot and bicycle patrol in the downtown core. [Presentation of internal raw data].
68 ConnexOntario: Addiction, Mental Health, and Problem Gambling Treatment Services. Mobile Crisis Response Program. (2020). Retrieved from: https://www.connexontario.ca/mental-health-service-sudbury-16552
69 Canadian Mental Health Association: Sudbury/Manitoulin. (2020). Community Mobilization Sudbury Rapid Mobilization Table. Retrieved from: https://sm.cmha.ca/ programs-services/community-mobilization-sudbury-cms/
70 Canadian Mental Health Association: Sudbury/Manitoulin. (2020). Harm Reduction Home Residential Program. Retrieved from: https://sm.cmha.ca/programs-services/harm-reduction-home-hrh-day-program/
71 Ontario Aboriginal HIV/AIDS Strategy. (2020). Retrieved from: https://www.oahas.org/about.html
72 Réseau ACCESS Network. (2020). Retrieved from: https://www.reseauaccessnetwork.com/
73 Shkagamik-Kwe Health Centre. (2020). Retrieved from: https://www.skhc.ca/ about-skhc/mission-vision/
74 Potier, C., Laprévote, V., Dubois-Arber, F., Cottencin, O., & Rolland, B. (2014). Supervised Consumption Services: what has been demonstrated? A systematic literature review. Drug and Alcohol Dependence, 145, 48–68. https://doi.org/10.1016/j.drugalcdep.2014.10.012
75 Kerr, T., Tyndall, M., Li, K., Montaner, J., & Wood, E. (2005). Safer injection facility use and syringe sharing in injection drug users. The Lancet, 366(9482), 316–318. Retrieved from https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(05)66475-6/fulltext
76 Wood, E., Tyndall, M. W., Lai, C., Montaner, J. S., & Kerr, T. (2006a). Impact of a medically supervised safer injecting facility on drug dealing and other drug-related crime. Substance Abuse Treatment, Prevention, and Policy, 1, 13. https://doi.org/10.1186/1747-597X-1-13
77 Kerr, T., Tyndall, M. W., Zhang, R., Lai, C., Montaner, J. S. G., & Wood, E. (2007). Circumstances of first injection among illicit drug users accessing a medically supervised safer injection facility. American Journal of Public Health, 97(7), 1228– 1230. https://doi.org/10.2105/AJPH.2006.086256
78 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/point-harm-reduction-supplies-services
79 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/point-harm-reduction-supplies-services
80 Public Health Sudbury & Districts. (2019). The Point (harm reduction supplies and services). Retrieved from https://www.phsd.ca/clinics-classes-events/ point-harm-reduction-supplies-services
81 Integrated Public Health Information System (iPHIS), Ministry of Health. Date Extracted: December, 2019.
82 Integrated Public Health Information System (iPHIS), Ministry of Health. Date Extracted: December, 2019.
83 Integrated Public Health Information System (iPHIS), Ministry of Health. Date Extracted: December, 2019.
84 Ontario Agency for Health Protection and Promotion (Public Health Ontario). (2019). Interactive Opioid Tool. Toronto, ON: Queen’s Printer for Ontario. Retrieved from: https://www.publichealthontario.ca/en/data-and-analysis/substance-use/interactive-opioid-tool
85 The Ontario Drug Policy Research Network (ODPRN). (2016). Opioid Use and Related Adverse Events in Ontario. Retrieved from https://odprn.ca/wp-content/uploads/2016/11/ODPRN-Opioid-Use-and-Related-Adverse-Events-Nov-2016.pdf
86 Ontario Agency for Health Protection and Promotion (Public Health Ontario). (2019). Interactive Opioid Tool. Toronto, ON: Queen’s Printer for Ontario. Retrieved from: https://www.publichealthontario.ca/en/data-and-analysis/substance-use/interactive-opioid-tool
87 Greater Sudbury Emergency Services Committee Report. (2019). Paramedic Services Opioid Surveillance and Reporting. Retrieved from https://agendasonline.greatersudbury.ca/index.cfm?pg=feed&action=file&agenda=report&itemid=7&id=1301&utm_source=sudbury.com&utm_campaign=sudbury.com&utm_medium=referral
88 Ontario Agency for Health Protection and Promotion (Public Health Ontario). (2019). Interactive Opioid Tool. Toronto, ON: Queen’s Printer for Ontario. Retrieved from: https://www.publichealthontario.ca/en/data-and-analysis/substance-use/interactive-opioid-tool
89 The Institute for Clinical Evaluative Sciences (ICES). (2017). Opioid Use Among First Nations in Ontario: A Report of Current Findings. Retrieved from https://www.ices.on.ca/About-ICES/Collaborations-and-Partnerships/Indigenous-Portfolio/Indigenous-Portfolio-Links
90 The Institute for Clinical Evaluative Sciences (ICES). (2017). Opioid Use Among First Nations in Ontario: A Report of Current Findings. Retrieved from https://www. ices.on.ca/About-ICES/Collaborations-and-Partnerships/Indigenous-Portfolio/Indigenous-Portfolio-Links
91 The Institute for Clinical Evaluative Sciences (ICES). (2017). Opioid Use Among First Nations in Ontario: A Report of Current Findings. Retrieved from https://www.ices.on.ca/About-ICES/Collaborations-and-Partnerships/Indigenous-Portfolio/Indigenous-Portfolio-Links
92 Reeves, A., & Stewart, S. L. (2014). Exploring the Integration of Indigenous Healing and Western Psychotherapy for Sexual Trauma Survivors Who Use Mental Health Services at Anishnawbe Health Toronto. Canadian Journal of Counselling and Psychotherapy, 49(1). Retrieved from https://cjc-rcc.ucalgary.ca/article/view/61008
93 Laurie, M. L., & Green, K. L. (2000). Health risks and opportunities for harm reduction among injection-drug-using clients of Saskatoon’s needle exchange program. Canadian Journal of Public Health, 91(5), 350-352.
94 Wood, E., Kerr, T., Small, W., Li, K., Marsh, D. C., Montaner, J. S. G., & Tyndall, M. W. (2004). Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. Canadian Medical Association Journal, 171(7), 731–734.
95 Stoltz, J.-A., Wood, E., Small, W., Li, K., Tyndall, M., Montaner, J., & Kerr, T. (2007). Changes in injecting practices associated with the use of a medically supervised safer injection facility. Journal of Public Health (Oxford, England), 29(1), 35–39. https://doi.org/10.1093/pubmed/fdl090
96 Wood, E., Tyndall, M. W., Montaner, J. S., & Kerr, T. (2006b). Summary of findings from the evaluation of a pilot medically supervised safer injecting facility. Canadian Medical Association Journal, 175(11), 1399–1404. https://doi.org/10.1503/ cmaj.060863
97 Hagan, H., Campbell, J. V., Thiede, H., Strathdee, S. A., Ouellet, L., Latka, M., … & DUIT Study Team. (2007). Injecting alone among young adult IDUs in five US cities: evidence of low rates of injection risk behavior. Drug and alcohol dependence, 91, S48-S55. https://dx.doi.org/10.1016%2Fj.drugalcdep.2007.02.002
98 Pinkerton, S. D. (2011). How many HIV infections are prevented by Vancouver Canada’s supervised injection facility? International Journal of Drug Policy, 22(3), 179–183. https://doi.org/10.1016/j.drugpo.2011.03.003
99 Marshall, B. D. L., Wood, E., Zhang, R., Tyndall, M. W., Montaner, J. S. G., & Kerr, T. (2009). Condom use among injection drug users accessing a supervised injecting facility. Sexually Transmitted Infections, 85(2), 121–126. https://doi.org/10.1136/ sti.2008.03252
100 Milloy, M.-J. S., Kerr, T., Zhang, R., Tyndall, M., Montaner, J., & Wood, E. (2009). Inability to access addiction treatment and risk of HIV infection among injection drug users recruited from a supervised injection facility. Journal of Public Health, 32(3), 342-349. https://doi.org/10.1093/pubmed/fdp089
101 Laurie, M. L., & Green, K. L. (2000). Health risks and opportunities for harm reduction among injection-drug-using clients of Saskatoon’s needle exchange program. Canadian Journal of Public Health, 91(5), 350-352.
102 British Columbia Centre on Substance Use (BCCSU). (2017). Supervised Consumption Services: Operational Guidance. Retrieved from https://www.bccsu.ca/ wp-content/uploads/2017/07/BC-SCS-Operational-Guidance.pdf
This item was last modified on March 3, 2025